

Prevalences of hyperuricemia and electrolyte abnormalities in patients with chronic kidney disease in Japan: A nationwide, cross-sectional cohort study using data from the Japan Chronic Kidney Disease Database (J-CKD-DB)
- PMID: 33057377
- PMCID: PMC7561156
- DOI: 10.1371/journal.pone.0240402
Prevalences of hyperuricemia and electrolyte abnormalities in patients with chronic kidney disease in Japan: A nationwide, cross-sectional cohort study using data from the Japan Chronic Kidney Disease Database (J-CKD-DB)
Abstract
Background: The Japan Chronic Kidney Disease Database (J-CKD-DB) is a nationwide clinical database of patients with chronic kidney disease (CKD) based on electronic health records. The objective of this study was to assess the prevalences of hyperuricemia and electrolyte abnormalities in Japanese patients with CKD.
Methods: In total, 35,508 adult outpatients with estimated glomerular filtration rates of 5-60 ml/min/1.73 m2 in seven university hospitals were included this analysis. The proportions of patients with CKD stages G3b, G4, and G5 were 23.5%, 7.6%, and 3.1%, respectively.
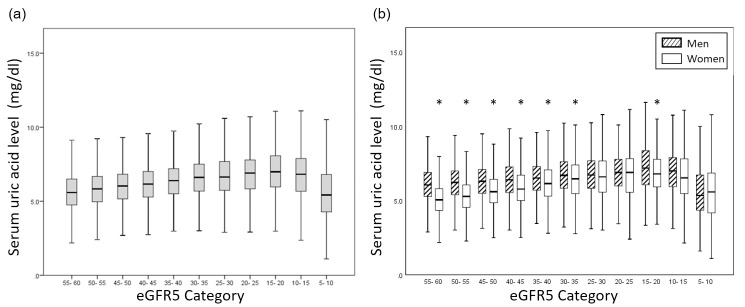
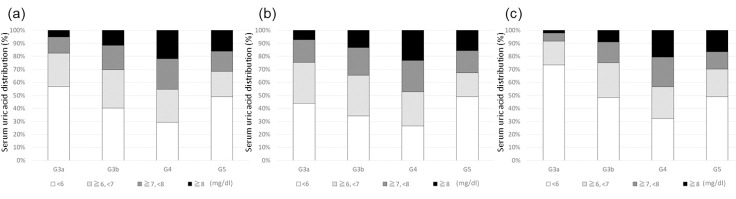
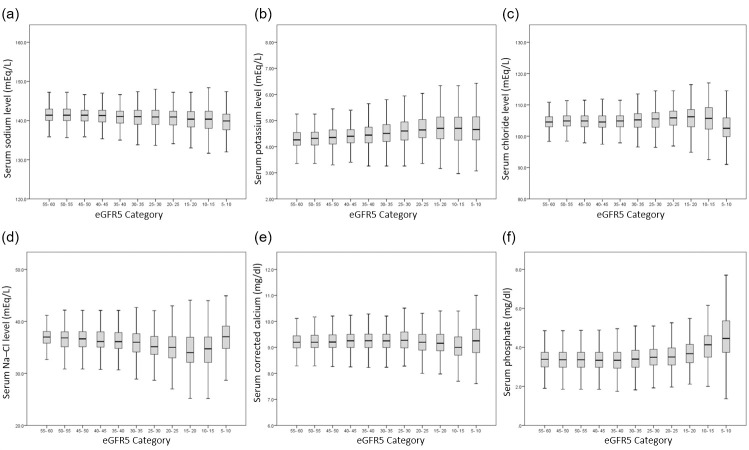
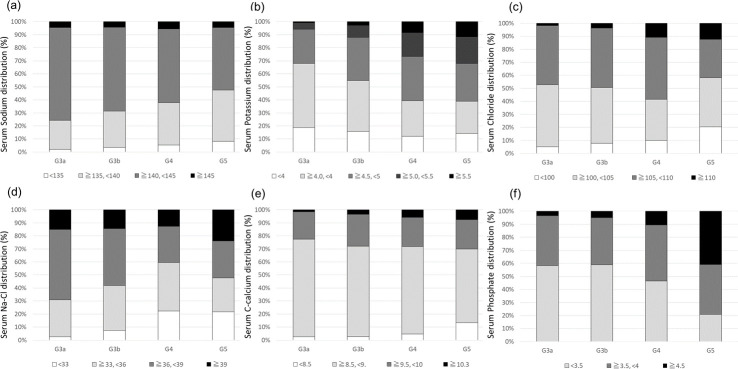
Results: Logistic regression analysis showed that prevalence of hyperuricemia was associated with CKD stages G3b (adjusted odds ratio [95% confidence interval]: 2.12 [1.90-2.37]), G4 (4.57 [3.92-5.32]), and G5 (2.25 [1.80-2.80]). The respective prevalences of hyponatremia, hypercalcemia, hyperphosphatemia, and narrower difference between serum sodium and chloride concentrations were elevated in patients with CKD stages G3b, G4, and G5, compared with those prevalences in patients with CKD stage G3a. The prevalences of hyperkalemia were 8.3% and 11.6% in patients with CKD stages G4 and G5, respectively. In patients with CKD stage G5, the proportions of patients with optimal ranges of serum uric acid, potassium, corrected calcium, and phosphate were 49.6%, 73.5%, 81.9%, and 56.1%, respectively.
Conclusions: We determined the prevalences of hyperuricemia and electrolyte abnormalities in Japanese patients with CKD using data from a nationwide cohort study.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39: S1–266. Available: http://www.ncbi.nlm.nih.gov/pubmed/11904577 - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108: 2154–69. 10.1161/01.CIR.0000095676.90936.80 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
