

Targeting myocardial ischaemic injury in the absence of reperfusion
- PMID: 33057804
- PMCID: PMC7560937
- DOI: 10.1007/s00395-020-00825-9
Targeting myocardial ischaemic injury in the absence of reperfusion
Abstract
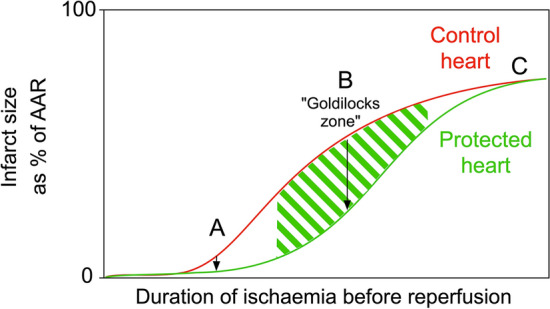
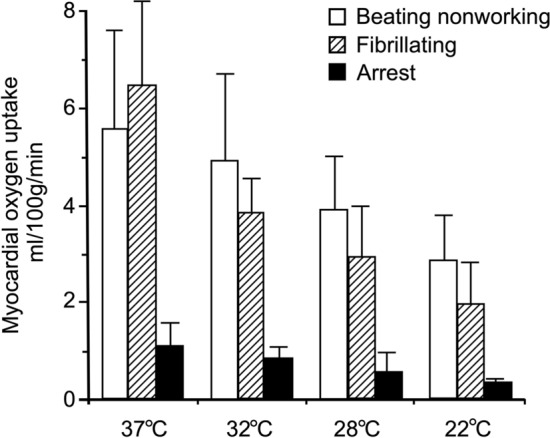
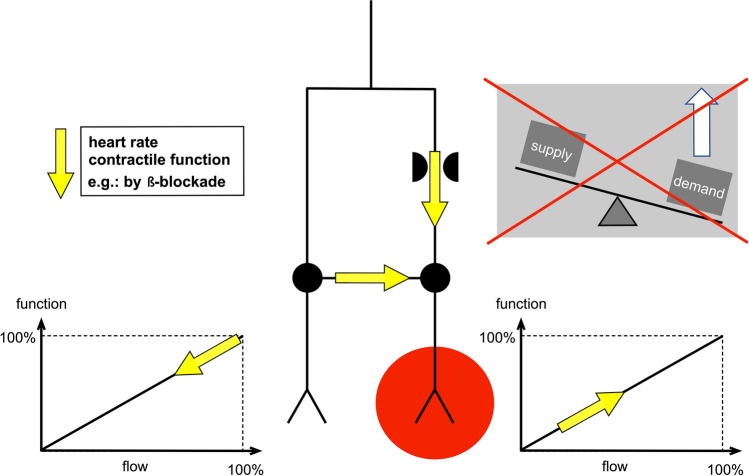
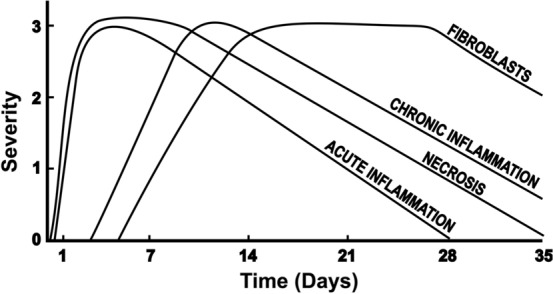
Sudden myocardial ischaemia causes an acute coronary syndrome. In the case of ST-elevation myocardial infarction (STEMI), this is usually caused by the acute rupture of atherosclerotic plaque and obstruction of a coronary artery. Timely restoration of blood flow can reduce infarct size, but ischaemic regions of myocardium remain in up to two-thirds of patients due to microvascular obstruction (MVO). Experimentally, cardioprotective strategies can limit infarct size, but these are primarily intended to target reperfusion injury. Here, we address the question of whether it is possible to specifically prevent ischaemic injury, for example in models of chronic coronary artery occlusion. Two main types of intervention are identified: those that preserve ATP levels by reducing myocardial oxygen consumption, (e.g. hypothermia; cardiac unloading; a reduction in heart rate or contractility; or ischaemic preconditioning), and those that increase myocardial oxygen/blood supply (e.g. collateral vessel dilation). An important consideration in these studies is the method used to assess infarct size, which is not straightforward in the absence of reperfusion. After several hours, most of the ischaemic area is likely to become infarcted, unless it is supplied by pre-formed collateral vessels. Therefore, therapies that stimulate the formation of new collaterals can potentially limit injury during subsequent exposure to ischaemia. After a prolonged period of ischaemia, the heart undergoes a remodelling process. Interventions, such as those targeting inflammation, may prevent adverse remodelling. Finally, harnessing of the endogenous process of myocardial regeneration has the potential to restore cardiomyocytes lost during infarction.
Keywords: Animals; Cardioprotection; Heart; Infarction; Ischaemia; Regeneration; Remodelling.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Ahn KT, Bin SY, Choe YH, Yang JH, Hahn JY, Choi JH, Choi SH, Chang SA, Lee SC, Lee SH, Oh JK, Gwon HC. Impact of transmural necrosis on left ventricular remodeling and clinical outcomes in patients undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. Int J Cardiovasc Imaging. 2013;29:835–842. doi: 10.1007/s10554-012-0155-9. - DOI - PubMed
-
- Arcari L, Cimino S, De Luca L, Francone M, Galea N, Reali M, Carbone I, Iacoboni C, Agati L. Impact of heart rate on myocardial salvage in timely reperfused patients with ST-segment elevation myocardial infarction: new insights from cardiovascular magnetic resonance. PLoS ONE. 2015;10:e0145495. doi: 10.1371/journal.pone.0145495. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
