

Role of imaging in visceral vascular emergencies
- PMID: 33057847
- PMCID: PMC7561664
- DOI: 10.1186/s13244-020-00913-3
Role of imaging in visceral vascular emergencies
Abstract
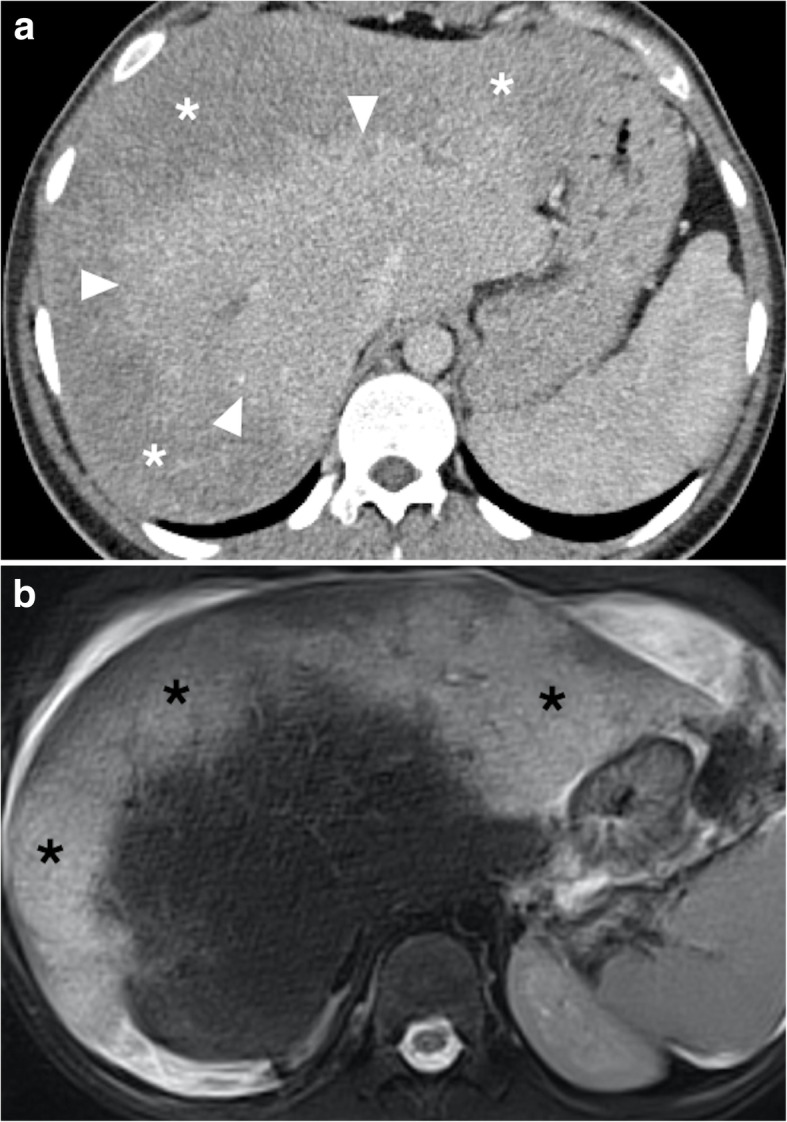
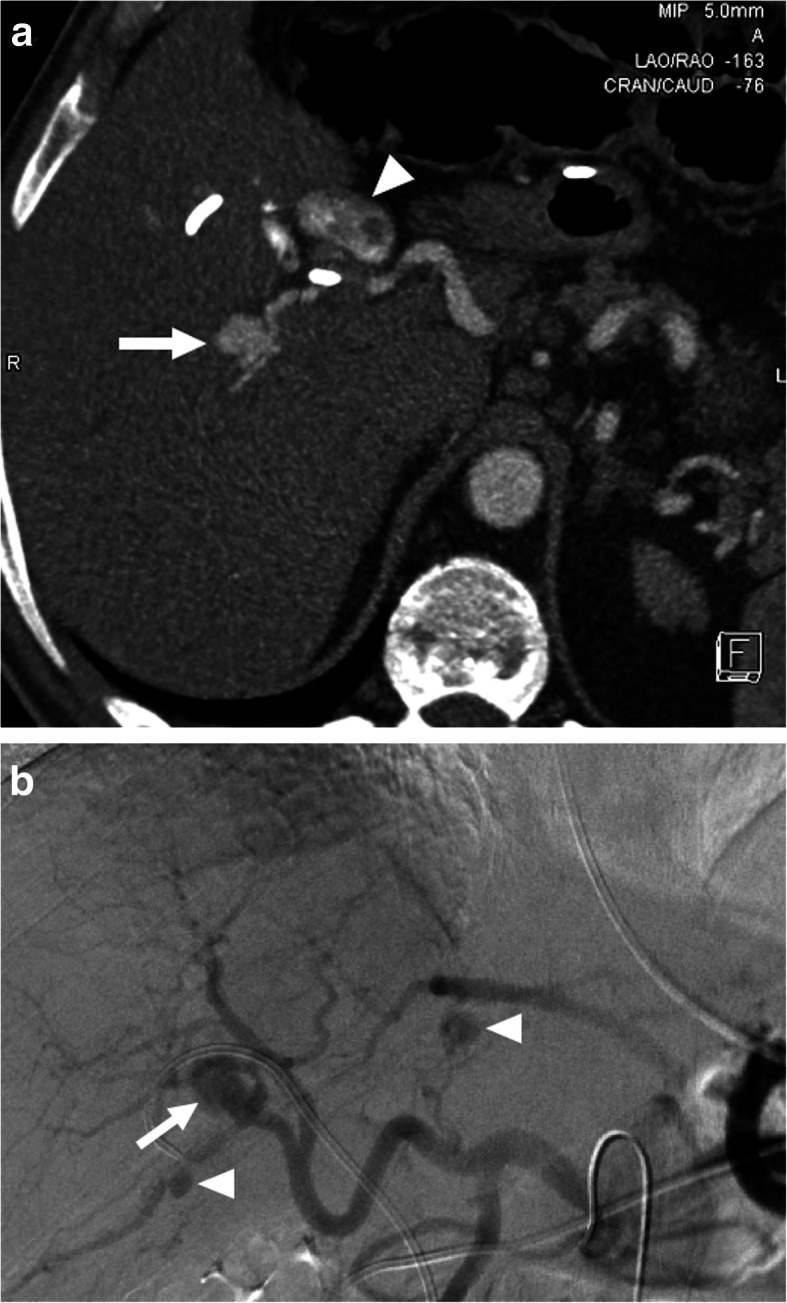
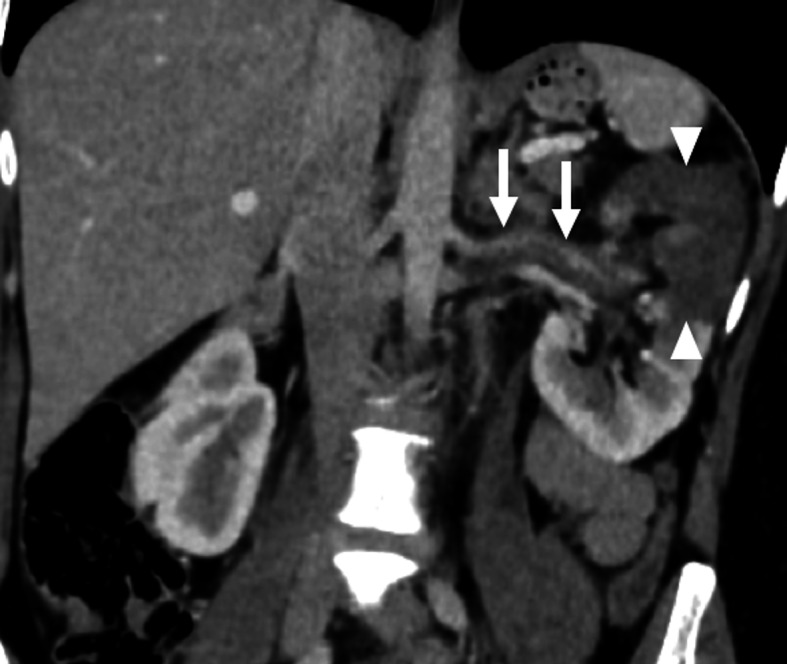
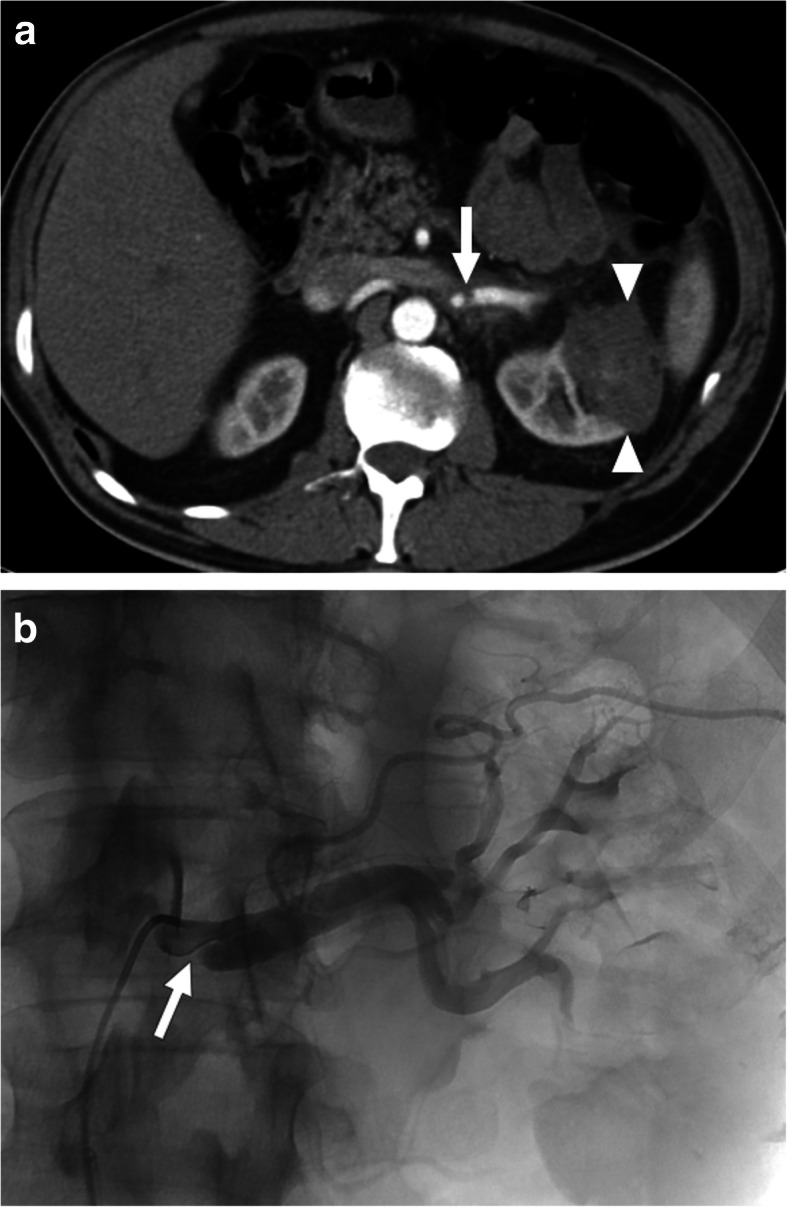
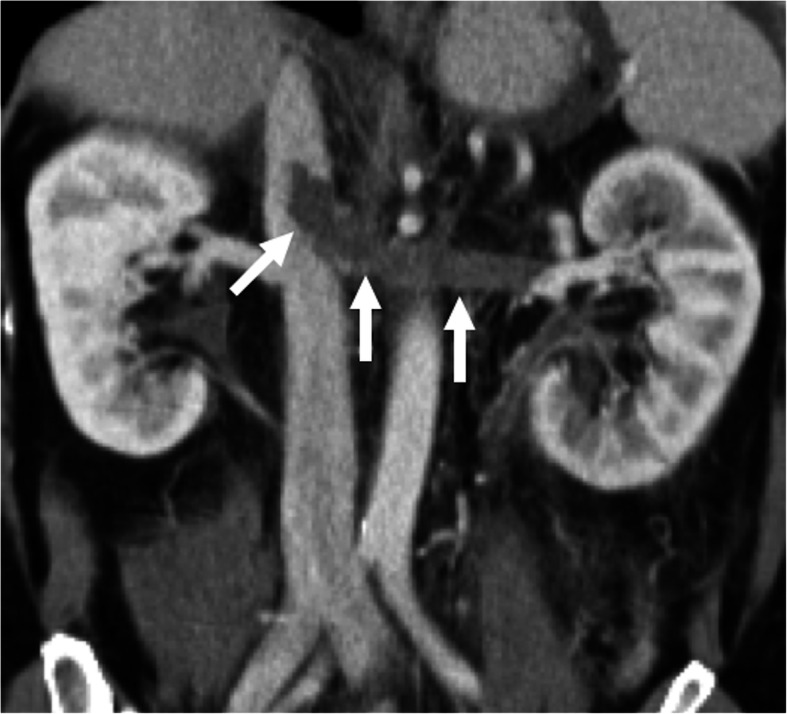
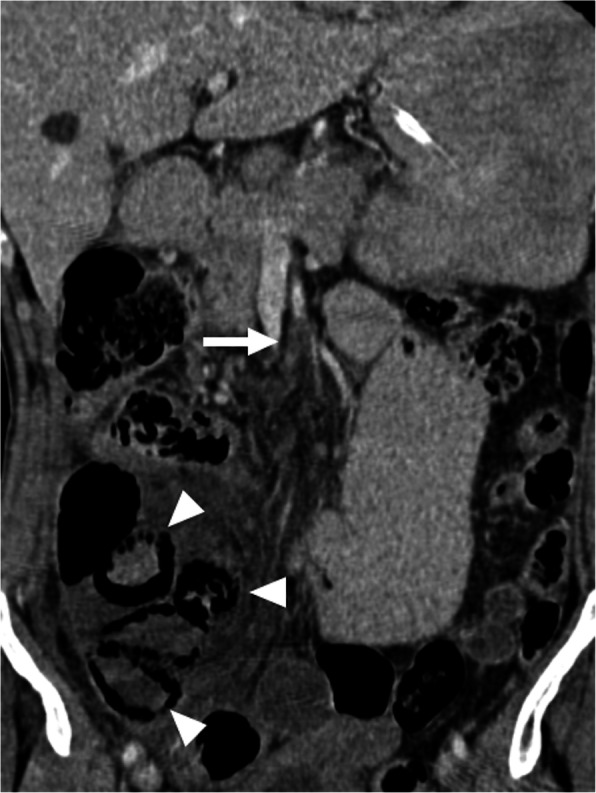
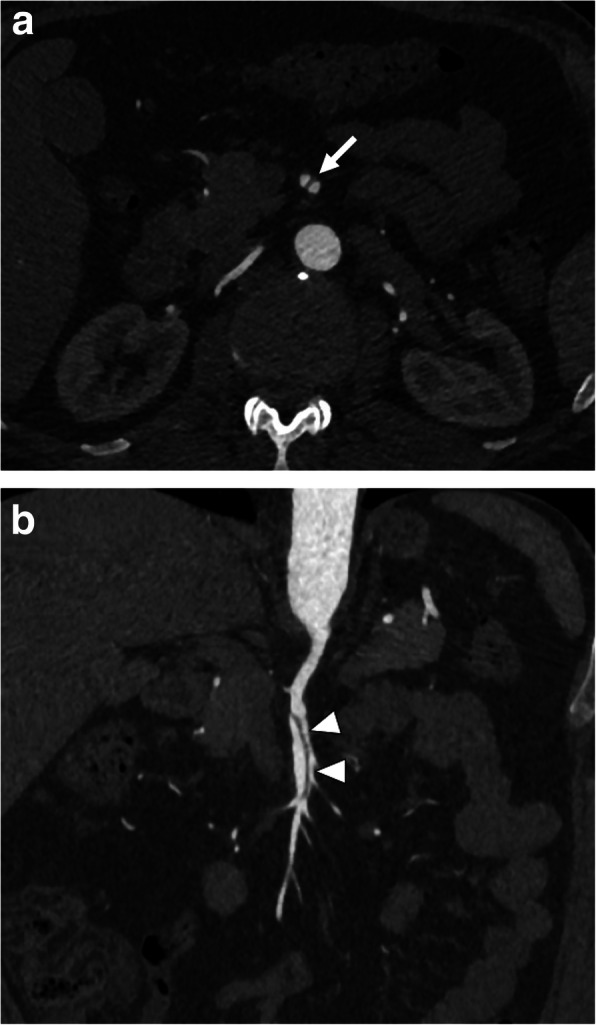
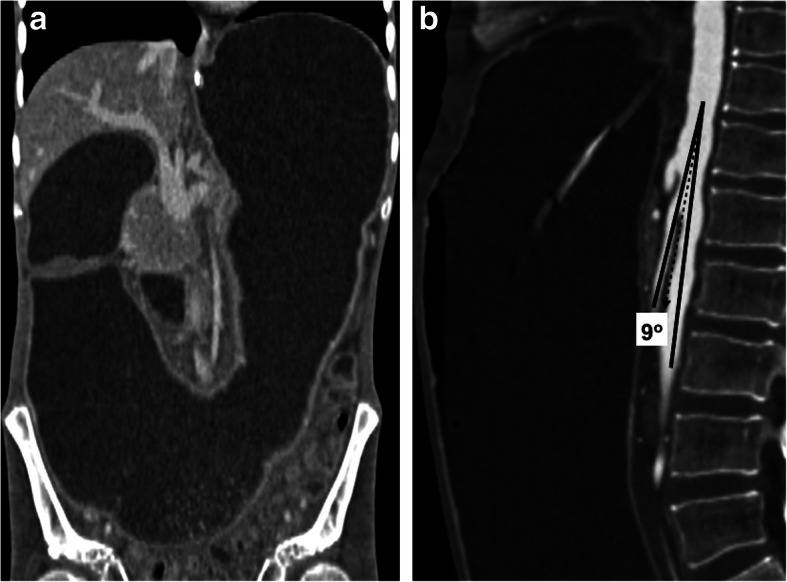
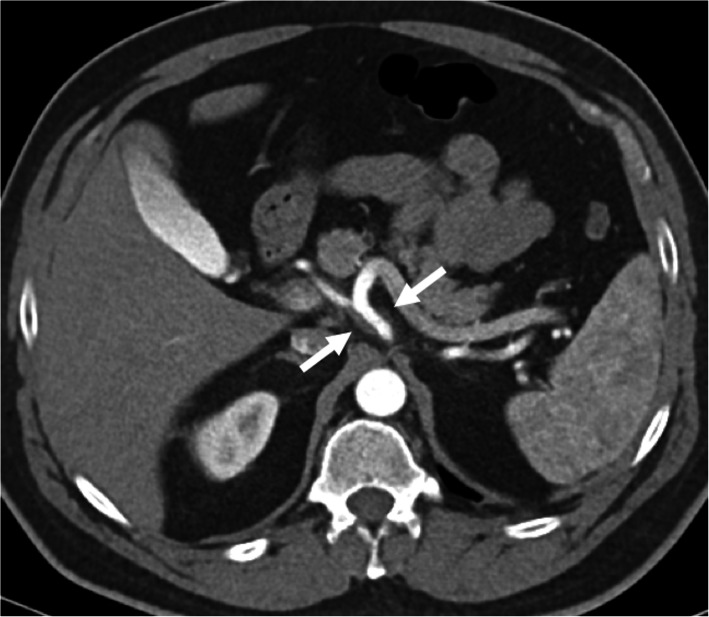
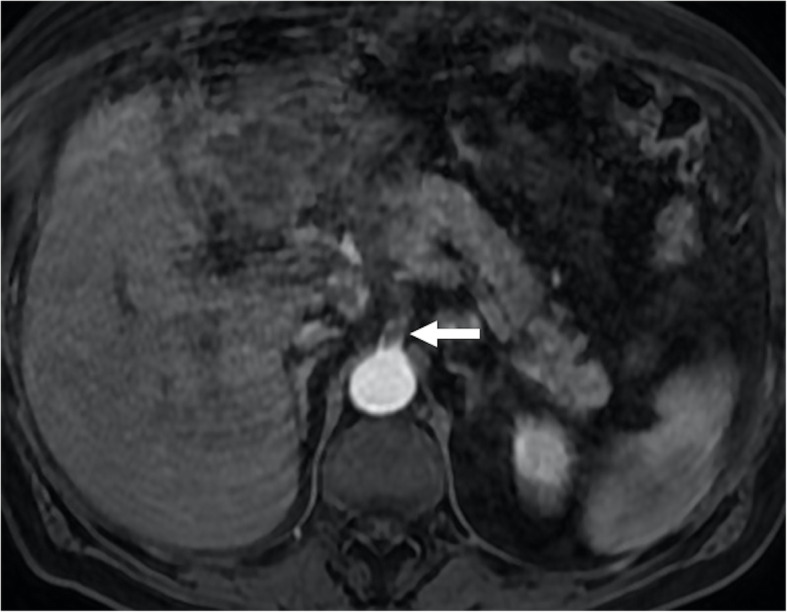
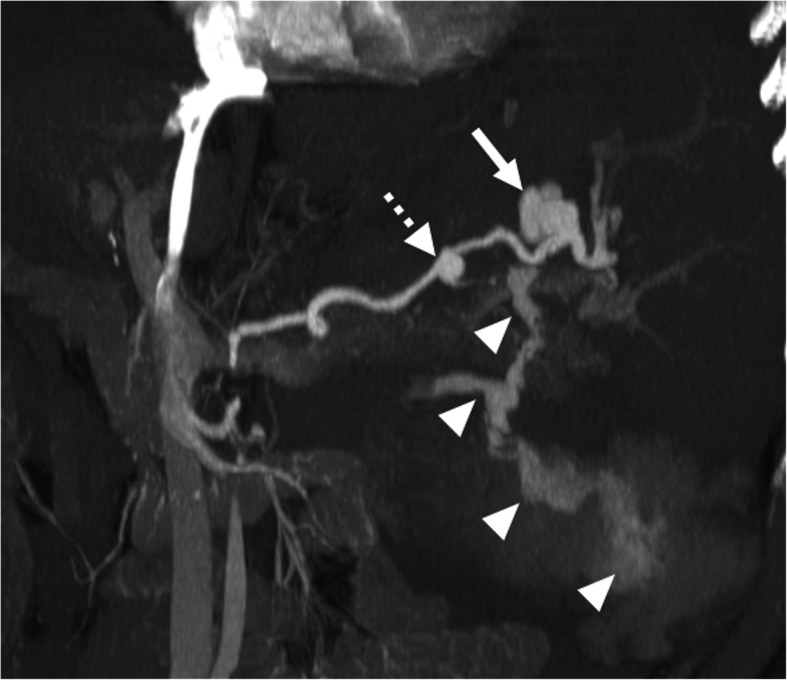
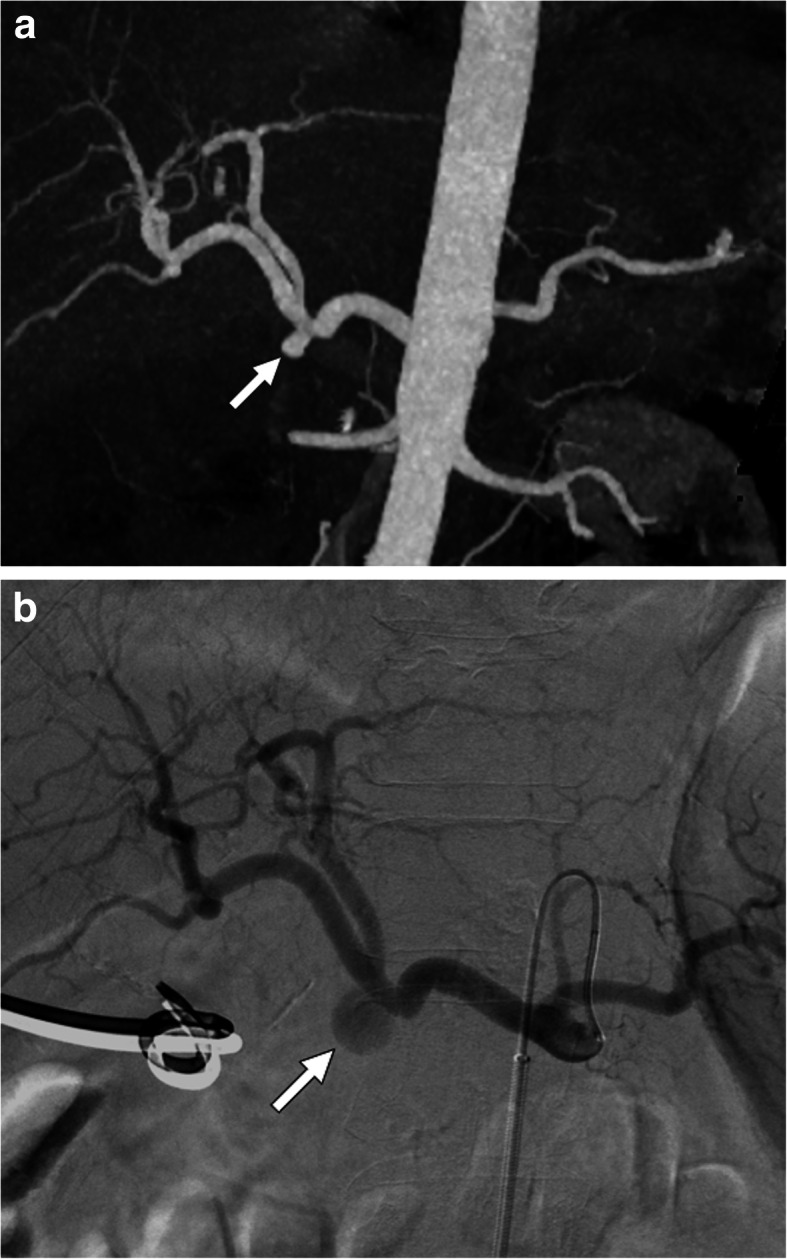
Differential diagnosis in non-traumatic acute abdomen is broad and unrelated diseases may simulate each other from a clinical perspective. Despite the fact that they are not as common, acute abdominal pain due to diseases related to visceral vessels may be life-threating if not detected and treated promptly. Thrombosis, dissection, and aneurysm in the abdominal visceral arteries or thrombosis in visceral veins may cause acute abdominal pain. Imaging with appropriate protocoling plays a fundamental role in both early diagnosis and determination of the treatment approach in these cases where early treatment can be life-saving. Computed tomography (CT) appears to be the most effective modality for the diagnosis as it provides high detail images in a very short time. Patient cooperation is also a less concern as compared to magnetic resonance imaging (MRI). As the imaging findings may sometimes be really subtle, diagnosis may be difficult especially to inexperienced imagers. Correct protocoling is also very critical to detect arterial abnormalities as visceral arterial abnormalities may not be detectable in portal phase only abdominal CT scans. In this article, we aimed to increase awareness among imaging specialists to these not very common causes of acute abdomen.
Keywords: Acute abdomen; Aneurysm; Dissection; Thrombosis; Vascular emergency; Visceral vessels.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures









References
-
- National Hospital Ambulatory Medical Care Survey: 2017 Emergency department summary tables [Internet]. U.S. Department of Health and Human Services • Centers for Disease Control and Prevention • National Center for Health Statistics. 2017. Available from: https://www.cdc.gov/nchs/data/nhamcs/web_tables/2017_ed_web_tables-508.pdf.
-
- Landry GJ, Yarmosh A, Liem TK et al (2018) Nonatherosclerotic vascular causes of acute abdominal pain. Am J Surg 215(5):838–841 - PubMed
-
- Plessier A, Darwish-Murad S, Hernandez-Guerra M et al (2010) Acute portal vein thrombosis unrelated to cirrhosis: a prospective multicenter follow-up study. Hepatology. 51(1):210–218 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
