

Graphical Presentations of Clinical Data in a Learning Electronic Medical Record
- PMID: 33058103
- PMCID: PMC7560537
- DOI: 10.1055/s-0040-1709707
Graphical Presentations of Clinical Data in a Learning Electronic Medical Record
Abstract
Background: Complex electronic medical records (EMRs) presenting large amounts of data create risks of cognitive overload. We are designing a Learning EMR (LEMR) system that utilizes models of intensive care unit (ICU) physicians' data access patterns to identify and then highlight the most relevant data for each patient.
Objectives: We used insights from literature and feedback from potential users to inform the design of an EMR display capable of highlighting relevant information.
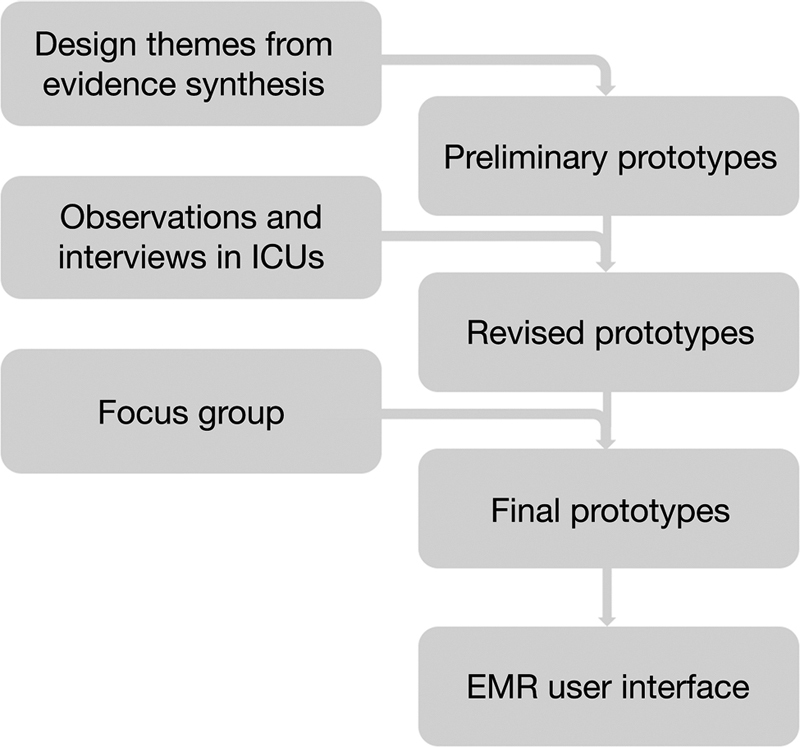
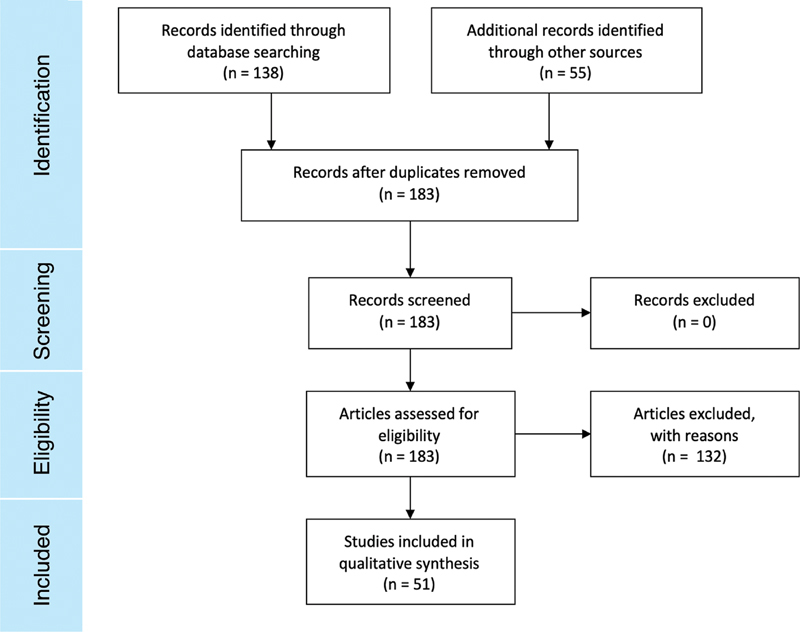
Methods: We used a review of relevant literature to guide the design of preliminary paper prototypes of the LEMR user interface. We observed five ICU physicians using their current EMR systems in preparation for morning rounds. Participants were interviewed and asked to explain their interactions and challenges with the EMR systems. Findings informed the revision of our prototypes. Finally, we conducted a focus group with five ICU physicians to elicit feedback on our designs and to generate ideas for our final prototypes using participatory design methods.
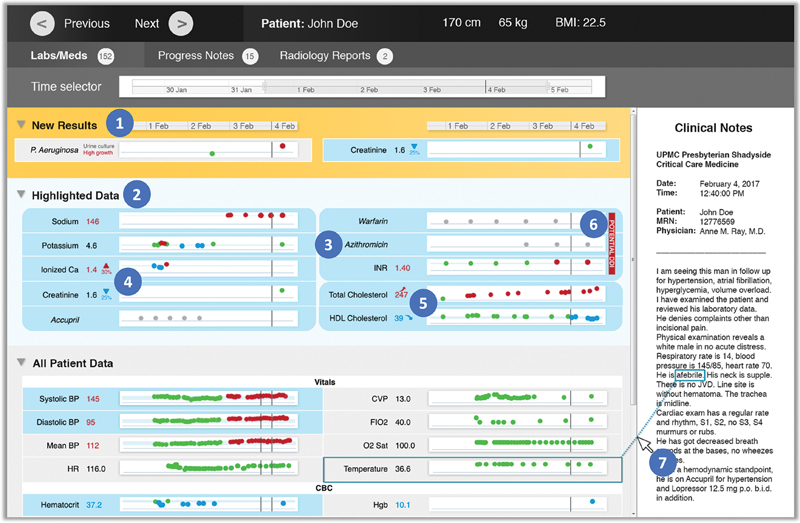
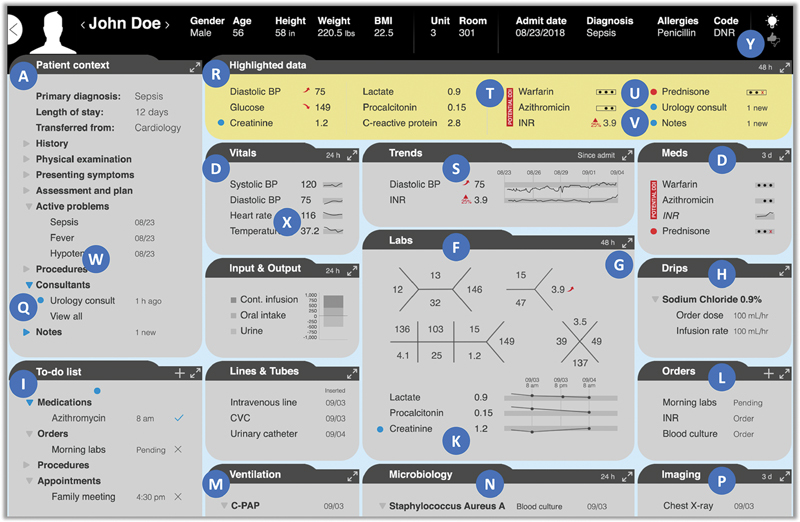
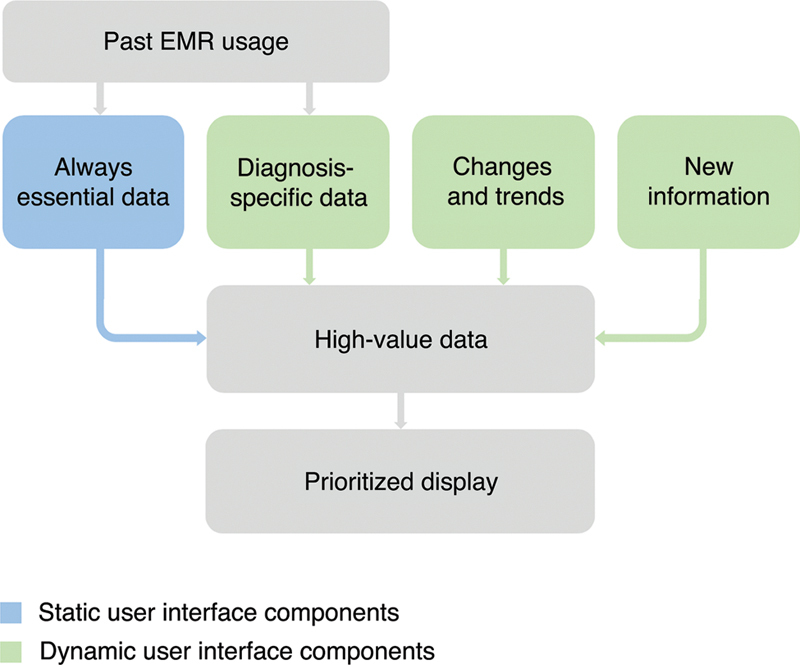
Results: Participating physicians expressed support for the LEMR system. Identified design requirements included the display of data essential for every patient together with diagnosis-specific data and new or significantly changed information. Respondents expressed preferences for fishbones to organize labs, mouseovers to access additional details, and unobtrusive alerts minimizing color-coding. To address the concern about possible physician overreliance on highlighting, participants suggested that non-highlighted data should remain accessible. Study findings led to revised prototypes, which will inform the development of a functional user interface.
Conclusion: In the feedback we received, physicians supported pursuing the concept of a LEMR system. By introducing novel ways to support physicians' cognitive abilities, such a system has the potential to enhance physician EMR use and lead to better patient outcomes. Future plans include laboratory studies of both the utility of the proposed designs on decision-making, and the possible impact of any automation bias.
Thieme. All rights reserved.
Conflict of interest statement
None declared.
Figures

Similar articles
-
Leveraging Eye Tracking to Prioritize Relevant Medical Record Data: Comparative Machine Learning Study.J Med Internet Res. 2020 Apr 2;22(4):e15876. doi: 10.2196/15876. J Med Internet Res. 2020. PMID: 32238342 Free PMC article.
-
Development and Preliminary Evaluation of a Prototype of a Learning Electronic Medical Record System.AMIA Annu Symp Proc. 2015 Nov 5;2015:1967-75. eCollection 2015. AMIA Annu Symp Proc. 2015. PMID: 26958296 Free PMC article.
-
Using machine learning to selectively highlight patient information.J Biomed Inform. 2019 Dec;100:103327. doi: 10.1016/j.jbi.2019.103327. Epub 2019 Oct 29. J Biomed Inform. 2019. PMID: 31676461 Free PMC article.
-
Usability and Safety in Electronic Medical Records Interface Design: A Review of Recent Literature and Guideline Formulation.Hum Factors. 2015 Aug;57(5):805-34. doi: 10.1177/0018720815576827. Epub 2015 Mar 23. Hum Factors. 2015. PMID: 25850118 Review.
-
Technology adoption of electronic medical records in developing economies: A systematic review on physicians' perspective.Digit Health. 2024 Jan 12;10:20552076231224605. doi: 10.1177/20552076231224605. eCollection 2024 Jan-Dec. Digit Health. 2024. PMID: 38222081 Free PMC article. Review.
Cited by
-
Engaging Multidisciplinary Clinical Users in the Design of an Artificial Intelligence-Powered Graphical User Interface for Intensive Care Unit Instability Decision Support.Appl Clin Inform. 2023 Aug;14(4):789-802. doi: 10.1055/s-0043-1775565. Epub 2023 Oct 4. Appl Clin Inform. 2023. PMID: 37793618 Free PMC article.
-
Human Factors and Organizational Issues in Health Informatics: Innovations and Opportunities.Yearb Med Inform. 2021 Aug;30(1):91-99. doi: 10.1055/s-0041-1726511. Epub 2021 Sep 3. Yearb Med Inform. 2021. PMID: 34479382 Free PMC article. Review.
-
Data Representation Structure to Support Clinical Decision-Making in the Pediatric Intensive Care Unit: Interview Study and Preliminary Decision Support Interface Design.JMIR Form Res. 2024 Feb 1;8:e49497. doi: 10.2196/49497. JMIR Form Res. 2024. PMID: 38300695 Free PMC article.
-
Building a Learning Health System: Creating an Analytical Workflow for Evidence Generation to Inform Institutional Clinical Care Guidelines.Appl Clin Inform. 2022 Jan;13(1):315-321. doi: 10.1055/s-0042-1743241. Epub 2022 Mar 2. Appl Clin Inform. 2022. PMID: 35235994 Free PMC article.
-
Involving Health Care Professionals in the Development of Electronic Health Records: Scoping Review.JMIR Hum Factors. 2023 Jul 10;10:e45598. doi: 10.2196/45598. JMIR Hum Factors. 2023. PMID: 37428524 Free PMC article.
References
-
- Hall A, Walton G. Information overload within the health care system: a literature review. Health Info Libr J. 2004;21(02):102–108. - PubMed
-
- Rind A. Interactive information visualization to explore and query Electronic Health Records. Found Trends Human–Computer Interact. 2013;5(03):207–298.