

Pulmonary Complications of Pediatric Hematopoietic Cell Transplantation. A National Institutes of Health Workshop Summary
- PMID: 33058742
- PMCID: PMC7919149
- DOI: 10.1513/AnnalsATS.202001-006OT
Pulmonary Complications of Pediatric Hematopoietic Cell Transplantation. A National Institutes of Health Workshop Summary
Abstract
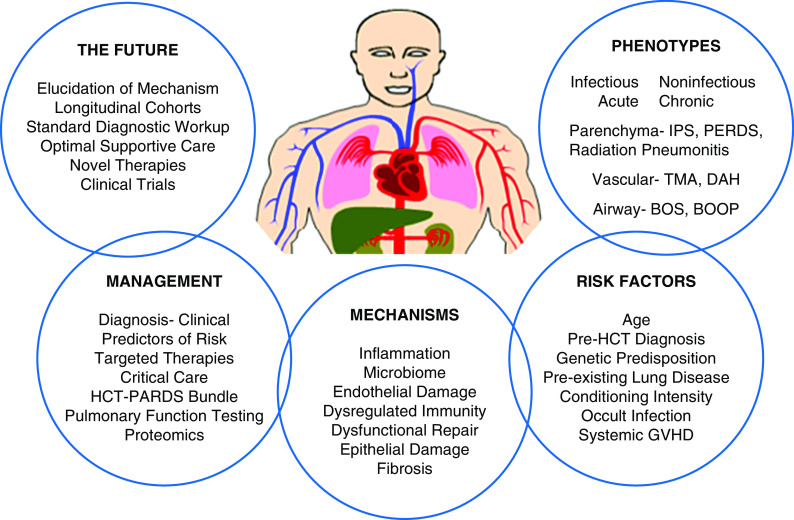
Approximately 2,500 pediatric hematopoietic cell transplants (HCTs), most of which are allogeneic, are performed annually in the United States for life-threatening malignant and nonmalignant conditions. Although HCT is undertaken with curative intent, post-HCT complications limit successful outcomes, with pulmonary dysfunction representing the leading cause of nonrelapse mortality. To better understand, predict, prevent, and/or treat pulmonary complications after HCT, a multidisciplinary group of 33 experts met in a 2-day National Institutes of Health Workshop to identify knowledge gaps and research strategies most likely to improve outcomes. This summary of Workshop deliberations outlines the consensus focus areas for future research.
Keywords: acute respiratory distress syndrome; hematopoietic cell transplantation; pediatrics; pulmonary complications; respiratory failure.
Figures



References
-
- Khandelwal P, Millard HR, Thiel E, Abdel-Azim H, Abraham AA, Auletta JJ, et al. Hematopoietic stem cell transplantation activity in pediatric cancer between 2008 and 2014 in the United States: a center for international blood and marrow transplant research report. Biol Blood Marrow Transplant. 2017;23:1342–1349. - PMC - PubMed
-
- Eikenberry M, Bartakova H, Defor T, Haddad IY, Ramsay NK, Blazar BR, et al. Natural history of pulmonary complications in children after bone marrow transplantation. Biol Blood Marrow Transplant. 2005;11:56–64. - PubMed
-
- Panoskaltsis-Mortari A, Griese M, Madtes DK, Belperio JA, Haddad IY, Folz RJ, et al. American Thoracic Society Committee on Idiopathic Pneumonia Syndrome. An official American Thoracic Society research statement: noninfectious lung injury after hematopoietic stem cell transplantation: idiopathic pneumonia syndrome. Am J Respir Crit Care Med. 2011;183:1262–1279. - PMC - PubMed
-
- Afessa B, Litzow MR, Tefferi A. Bronchiolitis obliterans and other late onset non-infectious pulmonary complications in hematopoietic stem cell transplantation. Bone Marrow Transplant. 2001;28:425–434. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
