

An Uncommon Lung Neoplasm in a Young Patient: Diagnostic Challenges
- PMID: 33060557
- PMCID: PMC7576687
- DOI: 10.12659/AJCR.926038
An Uncommon Lung Neoplasm in a Young Patient: Diagnostic Challenges
Abstract
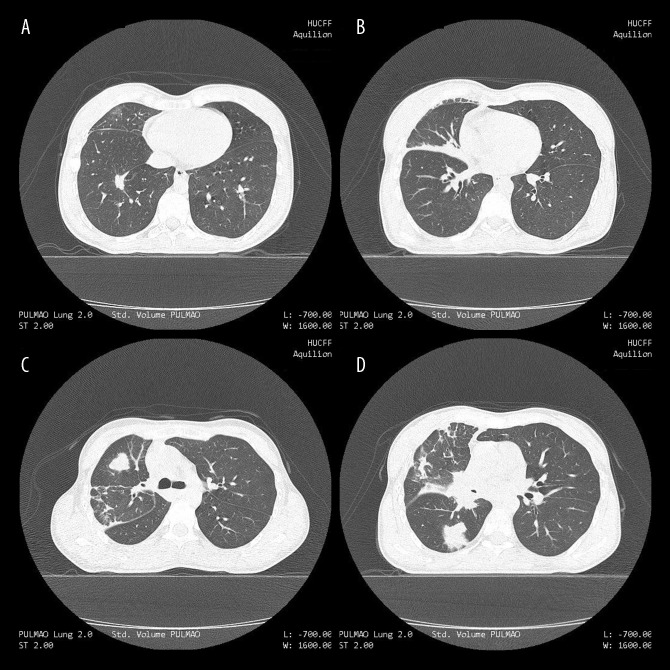
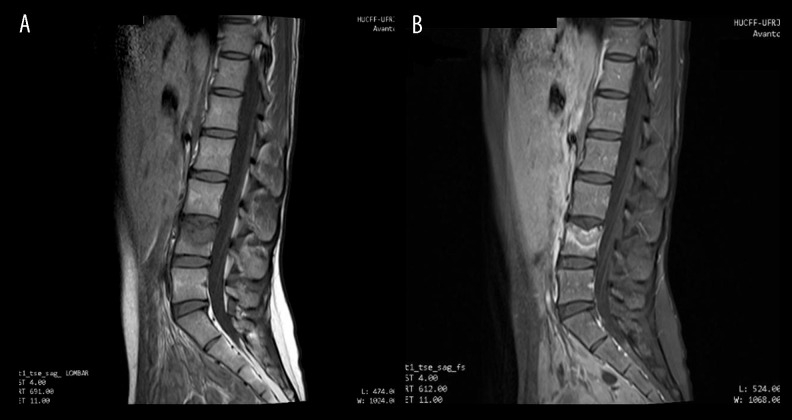
BACKGROUND Adenosquamous carcinoma of the lung (ASC) is a rare subtype of non-small-cell lung carcinoma (NSCLC), histologically defined by the presence of both squamous cell carcinoma and adenocarcinoma components. This aggressive malignancy has been rarely described in young female patients. Due to its low incidence and difficult-to-establish preoperative diagnosis, little is known about the complete clinical course for young patients with this specific NSCLC subtype. Moreover, a history of smoking is positively associated with ASC, but evidence for an association with exposure to secondhand smoke is sparse. CASE REPORT We present the case of a previously healthy 29-year-old woman with a long-standing history of secondhand smoke exposure, who was ultimately diagnosed with advanced ASC via fiberoptic bronchoscopy with transbronchial biopsy after a number of different investigations and treatments performed outside our service. She had visited many clinicians in 4 months of symptoms, initially presented as thoracic pain and cough thought to be due to a complicated pneumonia. Symptoms progressed despite empiric treatment and eventually included low back pain, weight loss, and night sweats. The hypothesis of tuberculosis was then investigated and discarded, at which point, 3 months after the onset of symptoms, she had a CT scan of the chest, revealing a pulmonary mass. She was referred to our hospital to further investigate this finding via fiberoptic bronchoscopy with transbronchial biopsy. During the procedure, she experienced an acute exacerbation of the low back pain, which prompted her admission in the Emergency Department, and she was later admitted to our pneumology ward. An extensive treatment plan including chemotherapy and radiotherapy was initially started, but could not be completed due to rapid disease progression, defined by pulmonary and spine metastatic implants, which limited treatment to palliative care. The patient died 6 months after the initial onset of symptoms. CONCLUSIONS This case report shows the clinical course of a difficult and rare diagnosis, and demonstrates the high level of suspicion required for the early diagnosis of lung neoplasms in young patients.
Conflict of interest statement
None.
Figures


Similar articles
-
Palliative Chemotherapy: Does It Only Provide False Hope? The Role of Palliative Care in a Young Patient With Newly Diagnosed Metastatic Adenocarcinoma.J Adv Pract Oncol. 2017 May-Jun;8(4):382-386. Epub 2017 May 1. J Adv Pract Oncol. 2017. PMID: 30018843 Free PMC article. Review.
-
A rare presentation of pulmonary sarcoidosis as a solitary lung mass: a case report.J Med Case Rep. 2018 Apr 13;12(1):94. doi: 10.1186/s13256-018-1632-0. J Med Case Rep. 2018. PMID: 29650028 Free PMC article.
-
Spontaneous remission of advanced progressive poorly differentiated non-small cell lung cancer: a case report and review of literature.BMC Pulm Med. 2019 Nov 11;19(1):210. doi: 10.1186/s12890-019-0978-4. BMC Pulm Med. 2019. PMID: 31711463 Free PMC article. Review.
-
Implantation of 125I radioactive seeds via c-TBNA combined with chemotherapy in an advanced non-small-cell lung carcinoma patient.BMC Pulm Med. 2019 Nov 8;19(1):205. doi: 10.1186/s12890-019-0974-8. BMC Pulm Med. 2019. PMID: 31703663 Free PMC article.
-
[A Case of Papillary Thyroid Cancer Diagnosed as Recurrent Pulmonary Metastases Diagnosed by Transbronchial Biopsies 18 Years After Surgery].J UOEH. 2020;42(4):353-358. doi: 10.7888/juoeh.42.353. J UOEH. 2020. PMID: 33268614 Japanese.
References
-
- Rao N. Adenosquamous carcinoma. Semin Diagn Pathol. 2014;31(4):271–77. - PubMed
-
- Travis WD, Brambilla E, Nicholson AG, et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015;10(9):1243–60. - PubMed
-
- Zhao H, Yang H, Yao F, et al. Improved survival associated with a balanced structure between adenomatous and squamous components in patients with adenosquamous carcinoma of the lung. Eur J Surg Oncol. 2016;42(11):1699–706. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
