

Aortitis and aortic aneurysm in systemic vasculitis
- PMID: 33061066
- PMCID: PMC7525910
- DOI: 10.1007/s12055-019-00832-z
Aortitis and aortic aneurysm in systemic vasculitis
Abstract
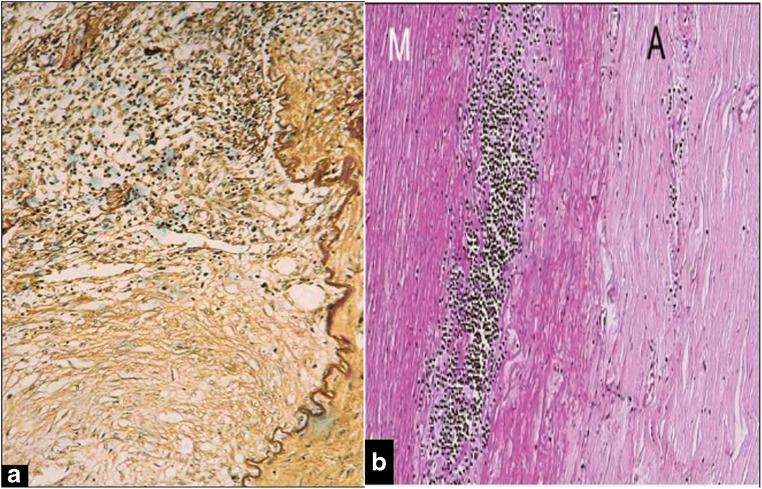
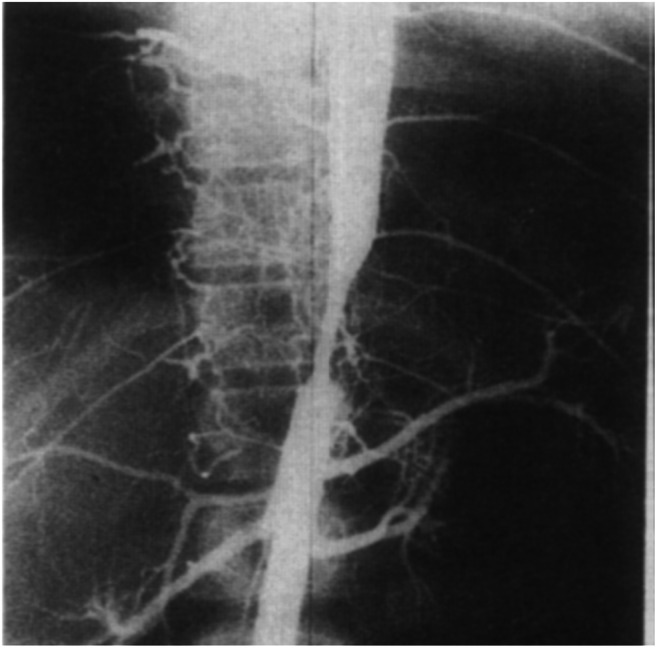
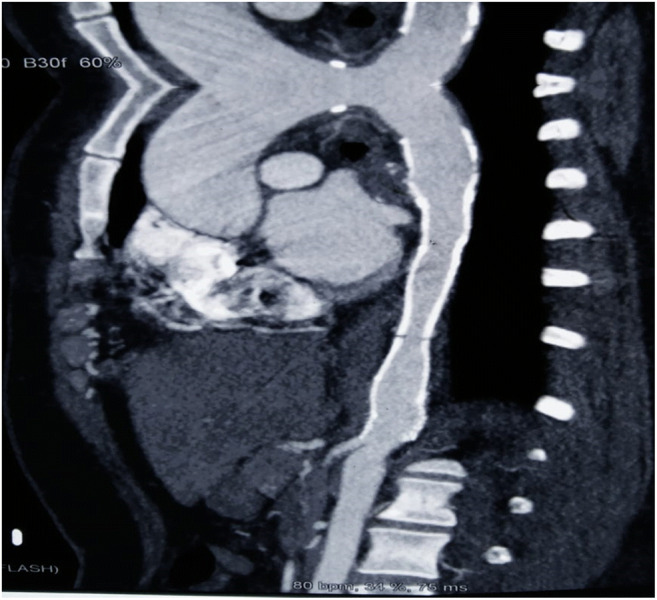
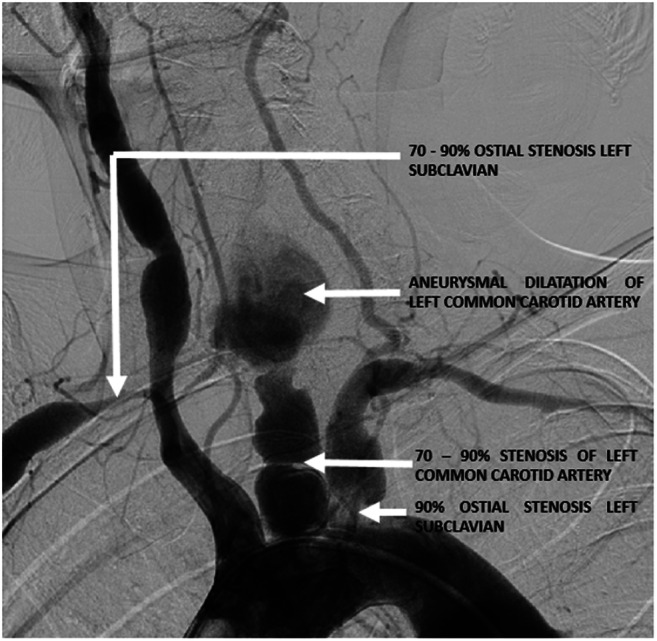
The term "large-vessel vasculitis" refers to chronic inflammation affecting the elastic arteries, mainly aorta and its major branches. Large-vessel vasculitis affecting the aorta is termed as "aortitis." This leads to diffuse wall thickening, loss of elasticity, stenosis, occlusion, dissection, calcification or aneurysm formation. Vasculitis involving the aorta includes Takayasu arteritis (commonest large-vessel vasculitis in India), giant cell arteritis (GCA), the periaortitis spectrum (including inflammatory abdominal aortic aneurysm), rheumatic diseases and IgG4-related disease. It is important for physicians to be aware of the aortic manifestations of common vasculitis-so that clinically relevant aortic involvement is not missed. Also, it is equally important for surgeons to keep in mind that aortic aneurysms can have an inflammatory aetiology. The primary reason for this is the central role that immunosuppressive therapy plays in the management of inflammatory aortic aneurysms. Surgical or percutaneous interventions, when needed, are most likely to succeed when performed after activity control; perioperative steroids may be beneficial in select cases, and postoperative disease activity control is imperative.
Keywords: Aortic aneurysm; Aortitis; Giant cell arteritis; Takayasu arteritis.
© Indian Association of Cardiovascular-Thoracic Surgeons 2019.
Conflict of interest statement
Conflicts of interestThe authors declare they have no conflict of interest.
Figures



References
-
- Loricera J, Blanco R, Hernández JL, et al. Non-infectious aortitis: a report of 32 cases from a single tertiary centre in a 4-year period and literature review. Clin Exp Rheumatol. 2015;33:S–19-31. - PubMed
-
- Miller DV, Isotalo PA, Weyand CM, Edwards WD, Aubry MC, Tazelaar HD. Surgical pathology of noninfectious ascending aortitis: a study of 45 cases with emphasis on an isolated variant. Am J Surg Pathol. 2006;30:1150–1158. doi: 10.1097/01.pas.0000213293.04026.ec. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources