

Aortic annulus and the importance of annuloplasty
- PMID: 33061189
- PMCID: PMC7525516
- DOI: 10.1007/s12055-019-00852-9
Aortic annulus and the importance of annuloplasty
Abstract
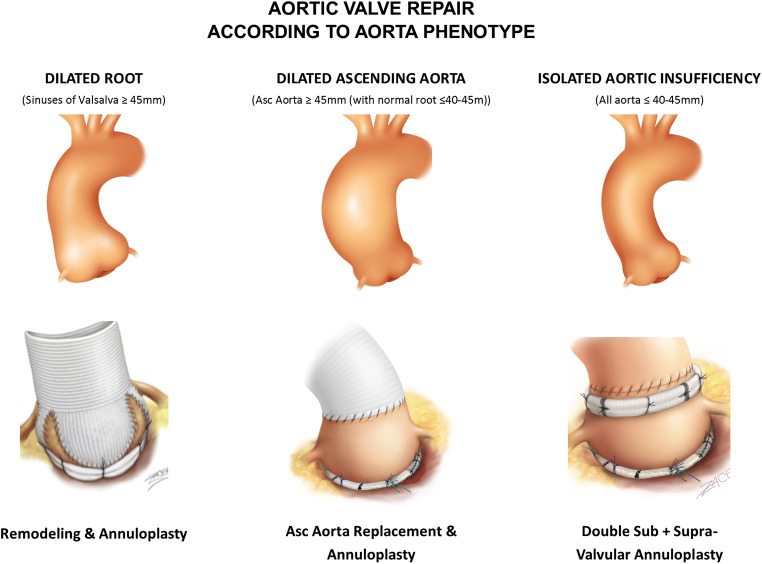
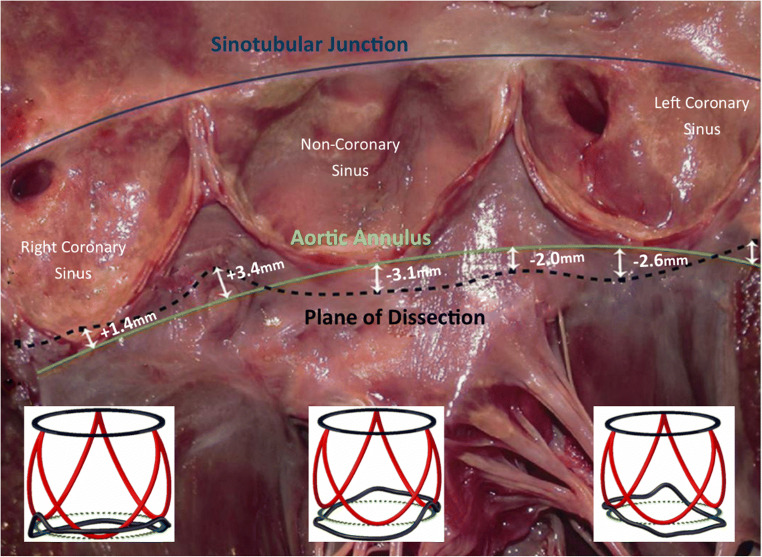
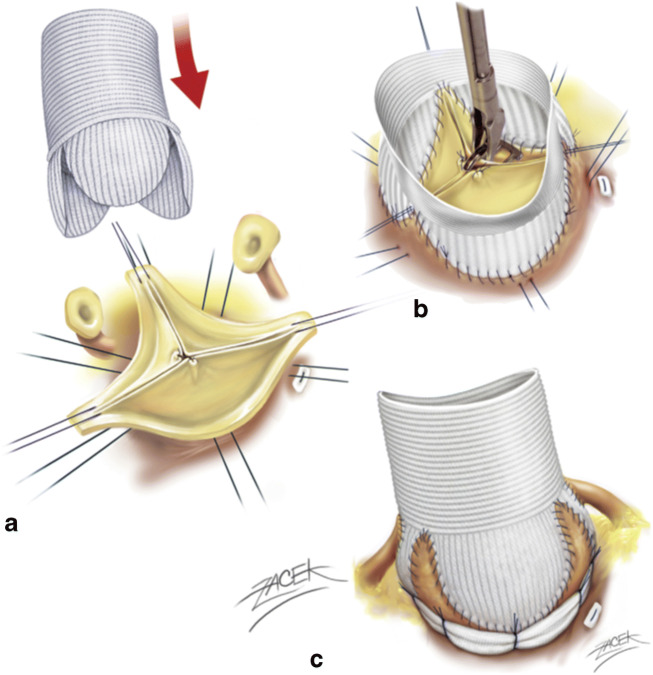
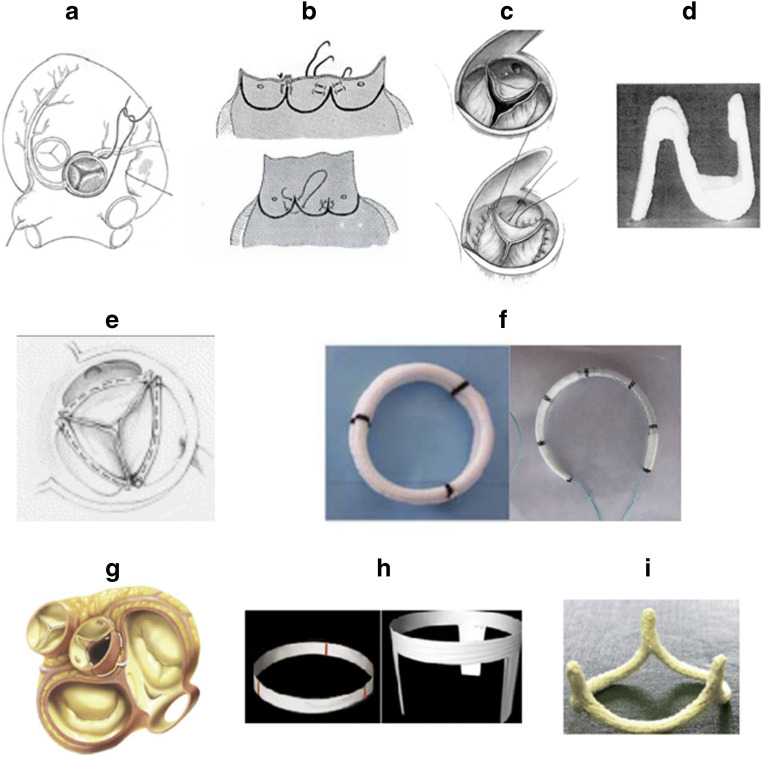
Dystrophic aortic insufficiency accounts for the majority of Western cases of aortic insufficiency and can be divided into the three phenotypes of isolated aortic insufficiency, dilated aortic root, and dilated ascending aorta. Each of these phenotypes is associated with a dilated annulus and/or sinotubular junction. Recent international guidelines recommend reimplantation or remodeling with aortic annuloplasty for valve-sparing root replacement, as well as consideration of aortic valve repair in cases of aortic insufficiency. A dilated aortic annulus is a major risk factor for failure of aortic valve repair procedures, indicating the need to address the annulus at the time of aortic valve or root repair. Calibrated annuloplasty should be performed at sub- and supravalular levels in order to restore the ratio of the sinotubular junction and annulus and be adapted according to the phenotype of the root and ascending aorta. Standardization of aortic valve repair techniques with use of a calibrated annuloplasty will improve dissemination of techniques and rate of aortic valve repair. Current medical evidence shows that aortic valve repair is safe, produces better quality of life, and reduces valve-related mortality compared to prosthetic valve replacement.
Keywords: Aneurysm; Aortic annuloplasty; Aortic insufficiency; Bicuspid; Remodeling; Valve repair; Valve sparing root replacement.
© Indian Association of Cardiovascular-Thoracic Surgeons 2019.
Conflict of interest statement
Conflict of interestThe authors declare that they have no conflict of interest.
Figures
References
-
- Falk V, Baumgartner H, Bax JJ, et al. 2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur J Cardiothorac Surg. 2017;52:616–664. - PubMed
-
- Schafers HJ, Raddatz A, Schmied W, et al. Reexamining remodeling. J Thorac Cardiovasc Surg. 2015;149:S30–S36. - PubMed
-
- Schneider U, Aicher D, Miura Y, Schafers HJ. Suture Annuloplasty in aortic valve repair. Ann Thorac Surg. 2016;101:783–785. - PubMed
-
- Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: the euro heart survey on Valvular heart disease. Eur Heart J. 2003;24:1231–1243. - PubMed
-
- Detaint D, Jondeau G. Dystrophic aortic insufficiency. Rev Prat. 2009;59:187–193. - PubMed
LinkOut - more resources
Full Text Sources