

How to improve adherence to antidepressant treatments in patients with major depression: a psychoeducational consensus checklist
- PMID: 33062034
- PMCID: PMC7552507
- DOI: 10.1186/s12991-020-00306-2
How to improve adherence to antidepressant treatments in patients with major depression: a psychoeducational consensus checklist
Abstract
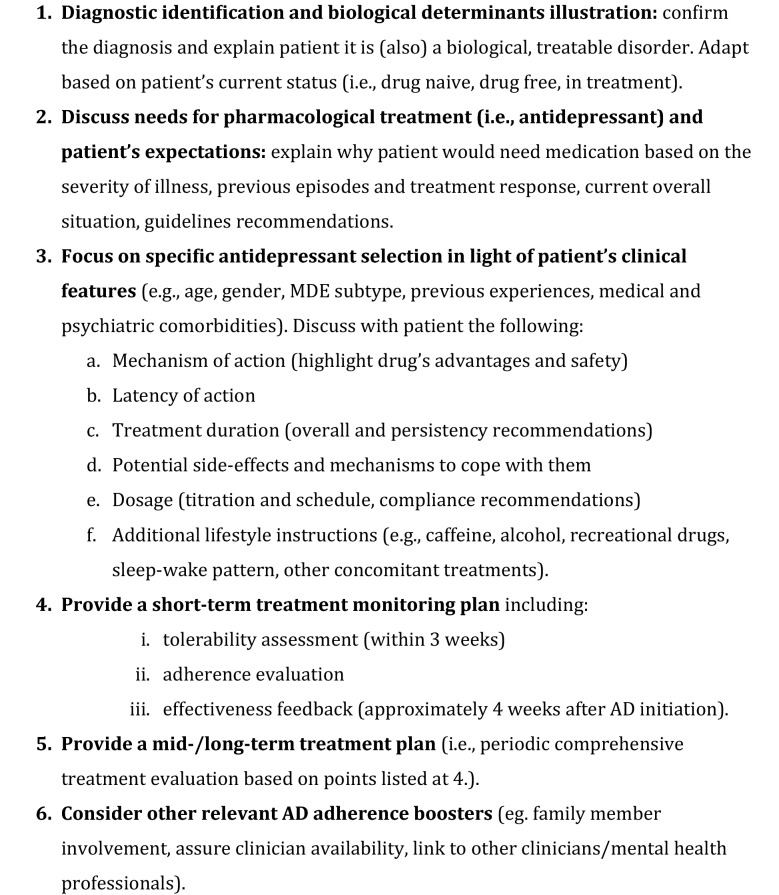
Studies conducted in primary care as well as in psychiatric settings show that more than half of patients suffering from major depressive disorder (MDD) have poor adherence to antidepressants. Patients prematurely discontinue antidepressant therapy for various reasons, including patient-related (e.g., misperceptions about antidepressants, side-effects, and lack of tolerability), clinician-related (e.g., insufficient instruction received by clinicians about the medication, lack of shared decision-making, and follow-up care), as well as structural factors (e.g., access, cost, and stigma). The high rate of poor adherence to antidepressant treatments provides the impetus for identifying factors that are contributing to noncompliance in an individual patient, to implement a careful education about this phenomenon. As adherence to antidepressants is one of the major unmet needs in MDD treatment, being associated with negative outcomes, we sought to identify a series of priorities to be discussed with persons with MDD with the larger aim to improve treatment adherence. To do so, we analyzed a series of epidemiological findings and clinical reasons for this phenomenon, and then proceeded to define through a multi-step consensus a set of recommendations to be provided by psychiatrists and other practitioners at the time of the first (prescription) visit with patients. Herein, we report the results of this initiative.
Keywords: Adherence; Antidepressants; Concordance; Consensus; Major depressive disorder.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsIn the last three years, Dr Dell’Osso has received lecture honoraria from Angelini, Lundbeck, Janssen, Pfizer, Neuraxpharm, Arcapharma, and Livanova; Dr Serafini received lecture honoraria from Neuraxpharm, Janssen-Cilag, Angelini, and Lundbeck; Dr Viganò has received lecture honoraria from Angelini, Lundbeck/Otsuka, and Gilead. In the last 3 years, Dr. Pompili has received lectures or advisory board honoraria or engaged in clinical trial activities with Angelini, Lundbeck, Janssen, Otsuka, Italfarmaco and Allergan, which are unrelated to this article. Other authors have none to declare.
Figures
References
-
- Forte A, Baldessarini RJ, Tondo L, Vázquez GH, Pompili M, Girardi P. Long-term morbidity in bipolar-I, bipolar-II, and unipolar major depressive disorders. J Affect Disord. 2015;178:71–78. - PubMed
-
- Van Der Voort TYG, Seldenrijk A, Van Meijel B, Goossens PJJ, Beekman ATF, Penninx BWJH, et al. Functional versus syndromal recovery in patients with major depressive disorder and bipolar disorder. J Clin Psychiatry. 2015;76(6):e809–e814. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
