

Renal Function is a Major Determinant of ICU-acquired Hypernatremia: A Balance Study on Sodium Handling
- PMID: 33062593
- PMCID: PMC7534501
- DOI: 10.2478/jtim-2020-0026
Renal Function is a Major Determinant of ICU-acquired Hypernatremia: A Balance Study on Sodium Handling
Abstract
Background and objectives: The development of ICU-acquired hypernatremia (IAH) is almost exclusively attributed to 'too much salt and too little water'. However, intrinsic mechanisms also have been suggested to play a role. To identify the determinants of IAH, we designed a prospective controlled study.
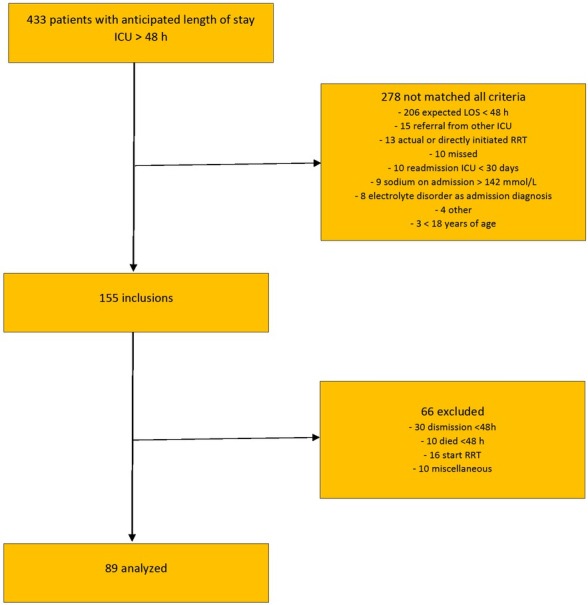
Methods: Patients with an anticipated length of stay ICU > 48 hours were included. Patients with hypernatremia on admission and/or on renal replacement therapy were excluded. Patients without IAH were compared with patients with borderline hypernatremia (≥ 143 mmol/L, IAH 143) and more severe hypernatremia (≥ 145 mmol/L, IAH 145).
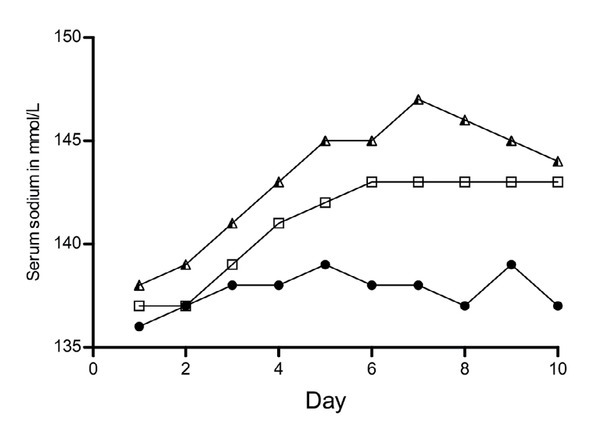
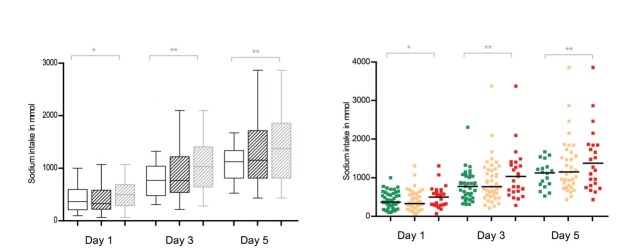
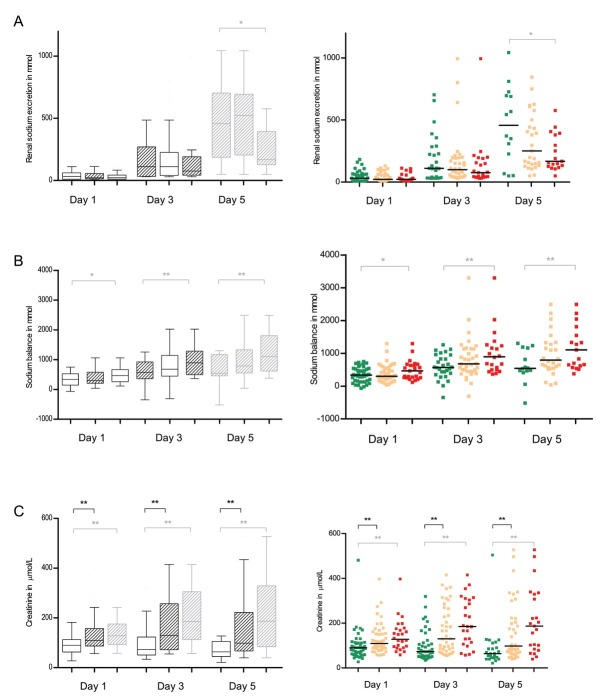
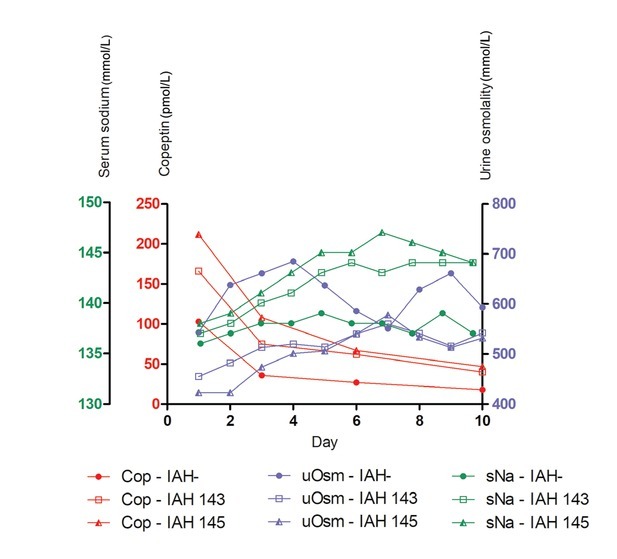
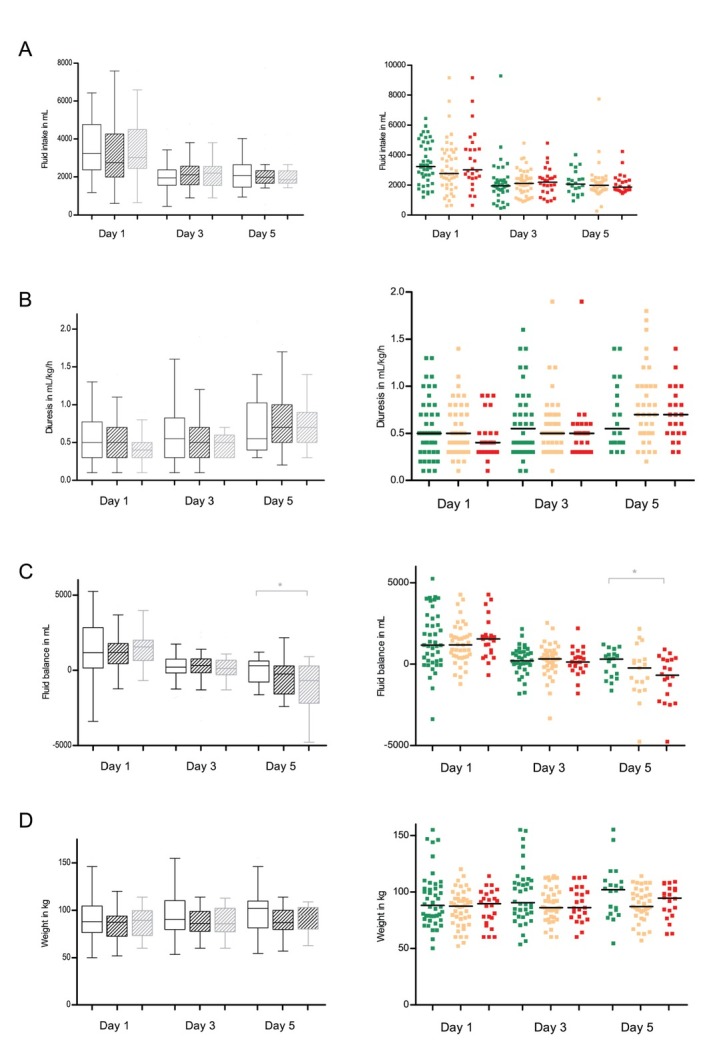
Results: We included 89 patients, of which 51% developed IAH 143 and 29% IAH 145. Sodium intake was high in all patients. Fluid balances were slightly positive and comparable between the groups. Patients with IAH 145 were more severely ill on admission, and during admission, their sodium intake, cumulative sodium balances, serum creatinine and copeptin levels were higher. According to the free water clearance, all the patients conserved water. On multivariate analysis, the baseline serum creatinine was an independent risk factor for the development of IAH 143 and IAH 145. Also, the copeptin levels remained significant for IAH 143 and IAH 145. Sodium intake remained only significant for patients with IAH 145.
Conclusions: Our data support the hypothesis that IAH is due to the combination of higher sodium intake and a urinary concentration deficit, as a manifestation of the renal impairment elicited by severe illness.
Keywords: ICU-patients; balance study; critically ill; electrolytes; hypernatremia; sodium handling.
© 2020 Marjolein van IJzendoorn, Linda de Vries, Jacob van den Born, Hanneke Buter, Gerjan Navis, Christiaan Boerma, published by Sciendo.
Conflict of interest statement
Conflict of Interest None of the authors have a conflict of interest.
Figures

References
-
- Polderman KH, Schreuder WO, Strack van Schijndel RJ, Thijs LG.. Hypernatremia in the intensive care unit: an indicator of quality of care? Crit Care Med. 1999;27:1105–8. - PubMed
-
- Darmon M, Timsit JF, Francais A, Nguile-Makao M, Adrie C, Cohen Y. Association between hypernatraemia acquired in the ICU and mortality: a cohort study. Nephrol Dial Transplant. 2010;25:2510–5. et al. - PubMed
-
- Lindner G, Funk GC, Schwarz C, Kneidinger N, Kaider A, Schneeweiss B. Hypernatremia in the critically ill is an independent risk factor for mortality. Am J Kidney Dis. 2007;50:952–7. et al. - PubMed
LinkOut - more resources
Full Text Sources