

Pathophysiologic Signatures of Bloodstream Infection in Critically Ill Adults
- PMID: 33063017
- PMCID: PMC7523775
- DOI: 10.1097/CCE.0000000000000191
Pathophysiologic Signatures of Bloodstream Infection in Critically Ill Adults
Abstract
Objectives: Bloodstream infection is associated with high mortality rates in critically ill patients but is difficult to identify clinically. This results in frequent blood culture testing, exposing patients to additional costs as well as the potential harms of unnecessary antibiotics. The purpose of this study was to assess whether the analysis of bedside physiologic monitoring data could accurately describe a pathophysiologic signature of bloodstream infection in patients admitted to the ICU.
Design: Development of a statistical model using physiologic data from a retrospective observational cohort.
Setting: University of Virginia Medical Center (Charlottesville, VA), a tertiary-care academic medical center.
Patients: Critically ill patients consecutively admitted to either the medical or surgical/trauma ICUs with available physiologic monitoring data between February 2011 and June 2015.
Interventions: None.
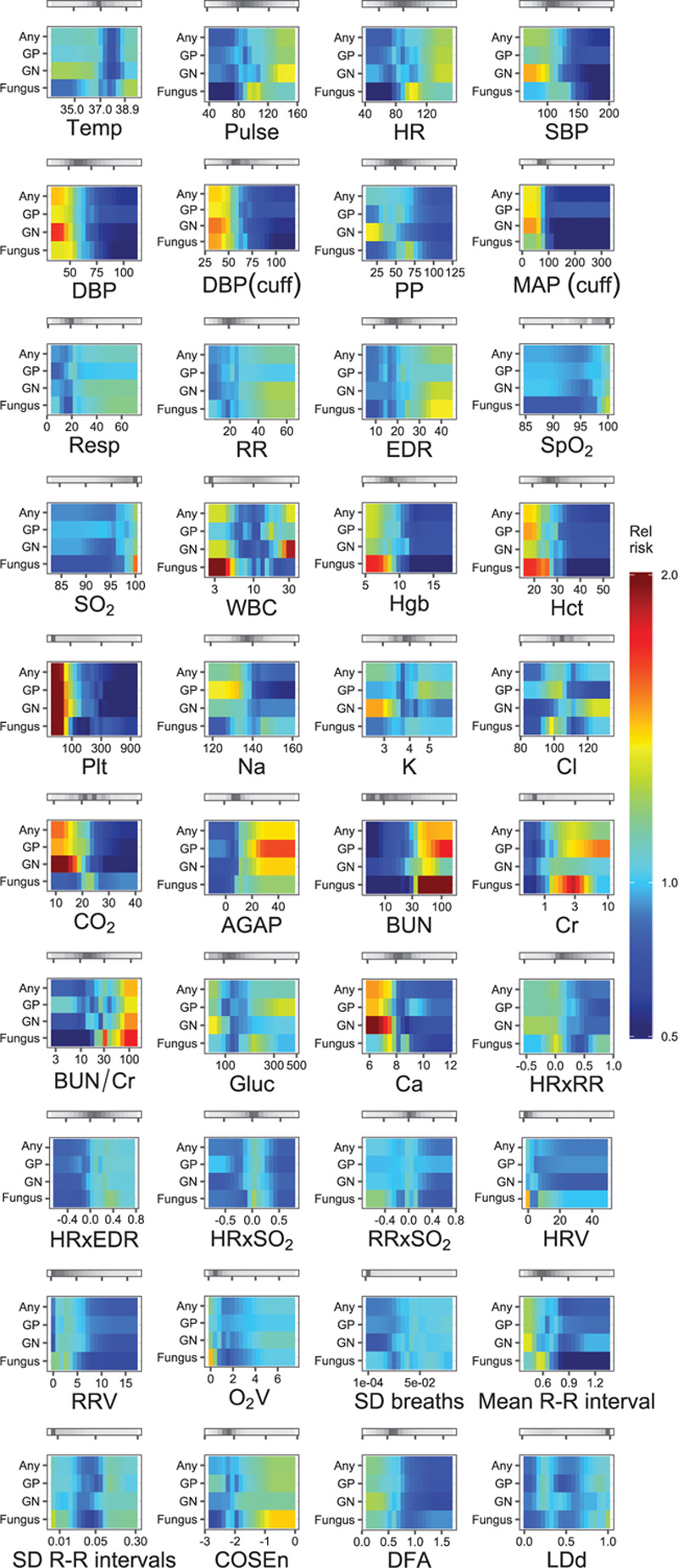
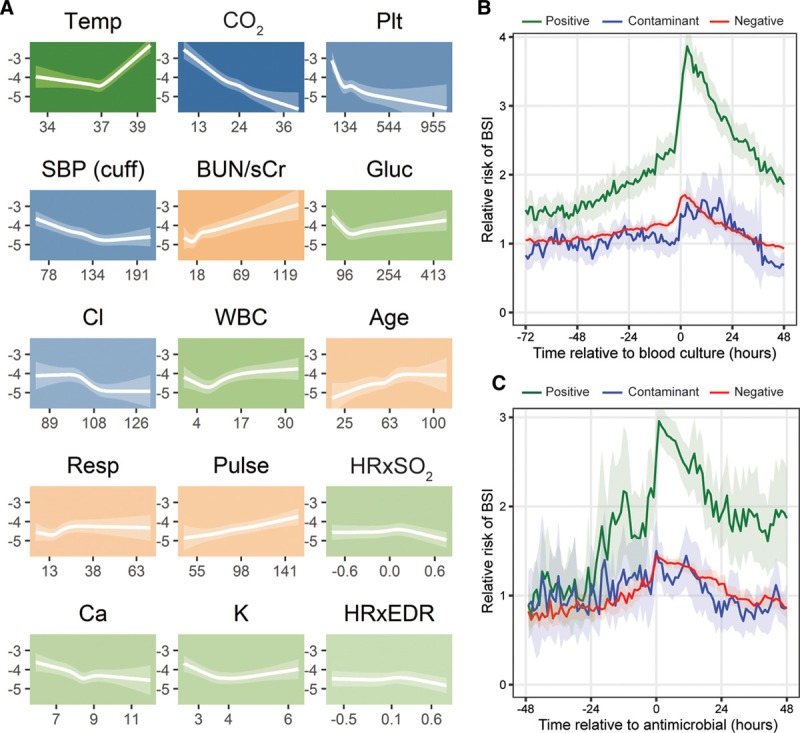
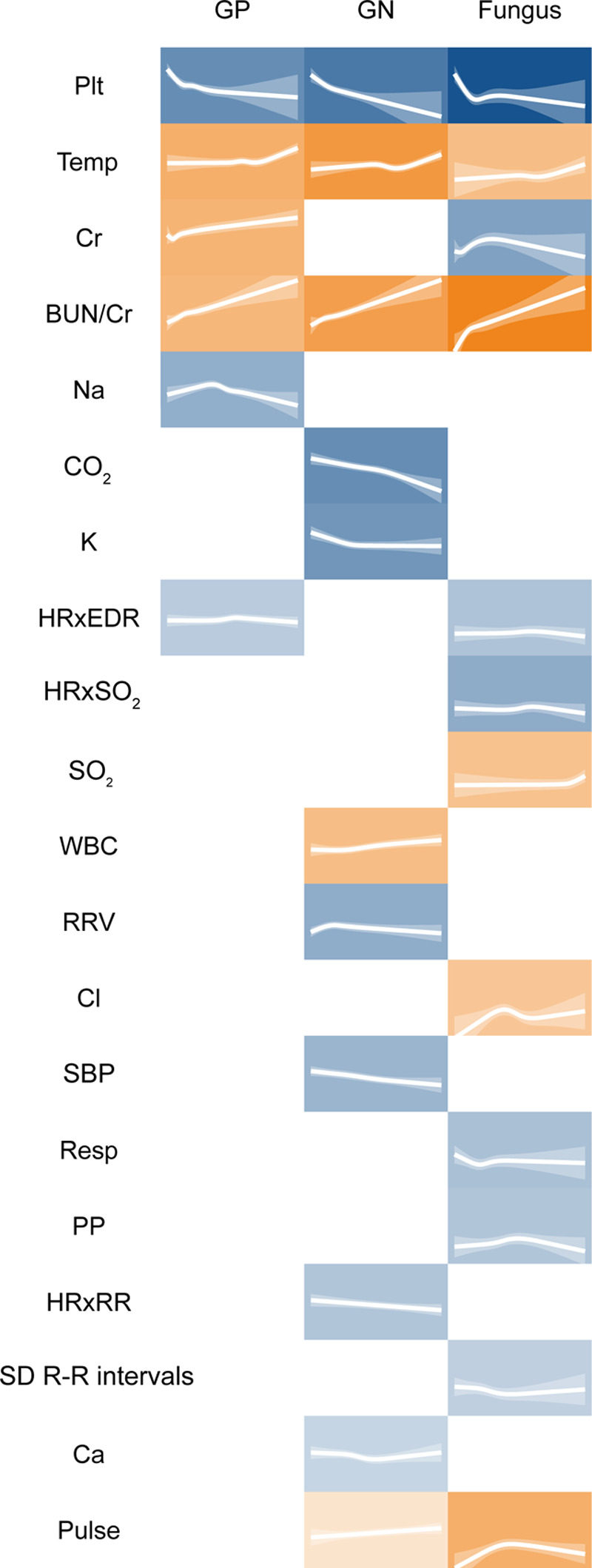
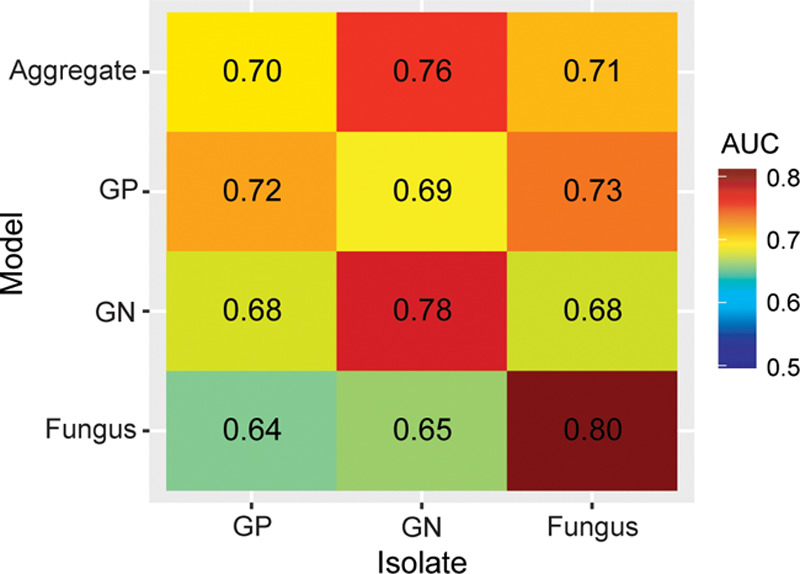
Measurements and main results: We analyzed 9,954 ICU admissions with 144 patient-years of vital sign and electrocardiography waveform data, totaling 1.3 million hourly measurements. There were 15,577 blood culture instances, with 1,184 instances of bloodstream infection (8%). The multivariate pathophysiologic signature of bloodstream infection was characterized by abnormalities in 15 different physiologic features. The cross-validated area under the receiver operating characteristic curve was 0.78 (95% CI, 0.69-0.85). We also identified distinct signatures of Gram-negative and fungal bloodstream infections, but not Gram-positive bloodstream infection.
Conclusions: Signatures of bloodstream infection can be identified in the routine physiologic monitoring data of critically ill adults. This may assist in identifying infected patients, maximizing diagnostic stewardship, and measuring the effect of new therapeutic modalities for sepsis.
Keywords: bacteremia; critical care; fungemia; physiologic monitoring; sepsis; statistical models.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Clark is employed by and holds equity in Advanced Medical Predictive Devices, Diagnostics, and Displays (AMP3D), Charlottesville, VA, which has licensed technologies from the University of Virginia Licensing and Ventures Group. Dr. Moorman is the chief medical officer of and holds equity in AMP3D. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Weinstein MP, Murphy JR, Reller LB, et al. The clinical significance of positive blood cultures: A comprehensive analysis of 500 episodes of bacteremia and fungemia in adults. II. Clinical observations, with special reference to factors influencing prognosis. Rev Infect Dis. 1983; 5:54–70 - PubMed
-
- Weinstein MP, Towns ML, Quartey SM, et al. The clinical significance of positive blood cultures in the 1990s: A prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults. Clin Infect Dis. 1997; 24:584–602 - PubMed
-
- Edgeworth JD, Treacher DF, Eykyn SJ. A 25-year study of nosocomial bacteremia in an adult intensive care unit. Crit Care Med. 1999; 27:1421–1428 - PubMed
-
- Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1994; 271:1598–1601 - PubMed
LinkOut - more resources
Full Text Sources
