

Higher mortality of COVID-19 in males: sex differences in immune response and cardiovascular comorbidities
- PMID: 33063089
- PMCID: PMC7665363
- DOI: 10.1093/cvr/cvaa284
Higher mortality of COVID-19 in males: sex differences in immune response and cardiovascular comorbidities
Abstract
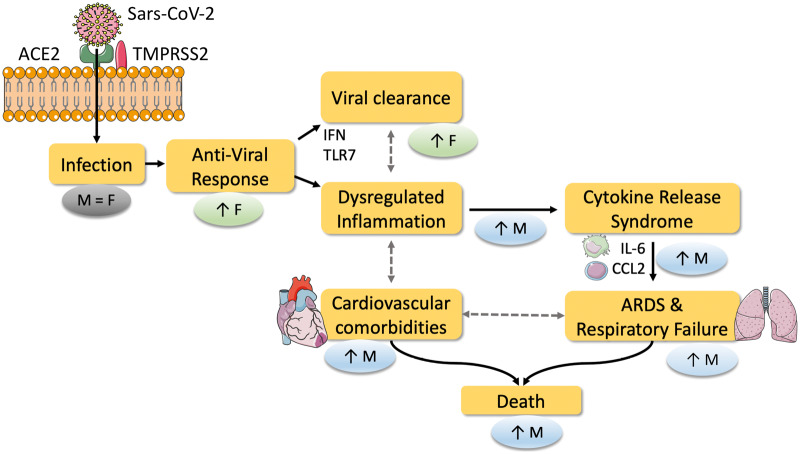
The high mortality rate of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection is a critical concern of the coronavirus disease 2019 (COVID-19) pandemic. Strikingly, men account for the majority of COVID-19 deaths, with current figures ranging from 59% to 75% of total mortality. However, despite clear implications in relation to COVID-19 mortality, most research has not considered sex as a critical factor in data analysis. Here, we highlight fundamental biological differences that exist between males and females, and how these may make significant contributions to the male-biased COVID-19 mortality. We present preclinical evidence identifying the influence of biological sex on the expression and regulation of angiotensin-converting enzyme 2 (ACE2), which is the main receptor used by SARS-CoV-2 to enter cells. However, we note that there is a lack of reports showing that sexual dimorphism of ACE2 expression exists and is of functional relevance in humans. In contrast, there is strong evidence, especially in the context of viral infections, that sexual dimorphism plays a central role in the genetic and hormonal regulation of immune responses, both of the innate and the adaptive immune system. We review evidence supporting that ineffective anti-SARS-CoV-2 responses, coupled with a predisposition for inappropriate hyperinflammatory responses, could provide a biological explanation for the male bias in COVID-19 mortality. A prominent finding in COVID-19 is the increased risk of death with pre-existing cardiovascular comorbidities, such as hypertension, obesity, and age. We contextualize how important features of sexual dimorphism and inflammation in COVID-19 may exhibit a reciprocal relationship with comorbidities, and explain their increased mortality risk. Ultimately, we demonstrate that biological sex is a fundamental variable of critical relevance to our mechanistic understanding of SARS-CoV-2 infection and the pursuit of effective COVID-19 preventative and therapeutic strategies.
Keywords: COVID-19; Cardiovascular comorbidities; Inflammation; SARS-CoV-2; Sex differences.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Guzik TJ, Mohiddin SA, Dimarco A, Patel V, Savvatis K, Marelli-Berg FM, Madhur MS, Tomaszewski M, Maffia P, D’Acquisto F, Nicklin SA, Marian AJ, Nosalski R, Murray EC, Guzik B, Berry C, Touyz RM, Kreutz R, Wang DW, Bhella D, Sagliocco O, Crea F, Thomson EC, McInnes IB. COVID-19 and the cardiovascular system: implications for risk assessment, diagnosis, and treatment options. Cardiovasc Res 2020;116:1666–1687. - PMC - PubMed
-
- Regitz-Zagrosek V, Kararigas G. Mechanistic pathways of sex differences in cardiovascular disease. Physiol Rev 2017;97:1–37. - PubMed
-
- COVID-19 sex-disaggregated data tracker—Global Health 50/50; https://globalhealth5050.org/covid19 (29 July 2020, date last accessed).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
