

Cardiac magnetic resonance T2 mapping and feature tracking in athlete's heart and HCM
- PMID: 33063183
- PMCID: PMC8043946
- DOI: 10.1007/s00330-020-07289-4
Cardiac magnetic resonance T2 mapping and feature tracking in athlete's heart and HCM
Abstract
Objectives: Distinguishing hypertrophic cardiomyopathy (HCM) from left ventricular hypertrophy (LVH) due to systematic training (athlete's heart, AH) from morphologic assessment remains challenging. The purpose of this study was to examine the role of T2 mapping and deformation imaging obtained by cardiovascular magnetic resonance (CMR) to discriminate AH from HCM with (HOCM) or without outflow tract obstruction (HNCM).
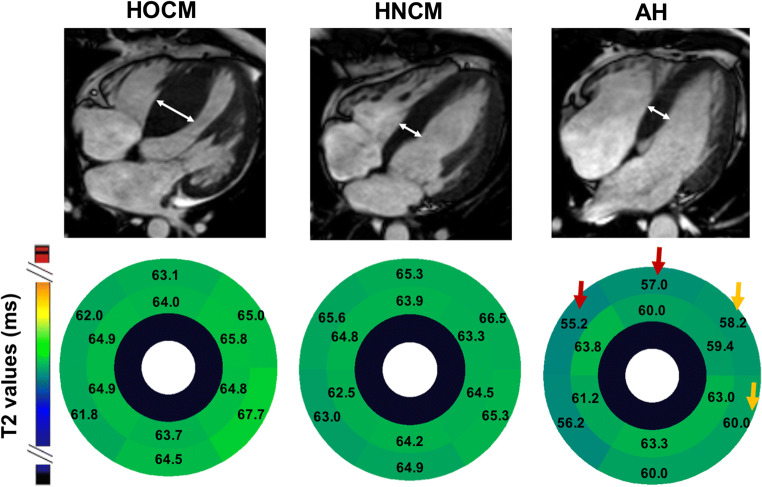
Methods: Thirty-three patients with HOCM, 9 with HNCM, 13 strength-trained athletes as well as individual age- and gender-matched controls received CMR. For T2 mapping, GRASE-derived multi-echo images were obtained and analyzed using dedicated software. Besides T2 mapping analyses, left ventricular (LV) dimensional and functional parameters were obtained including LV mass per body surface area (LVMi), interventricular septum thickness (IVS), and global longitudinal strain (GLS).
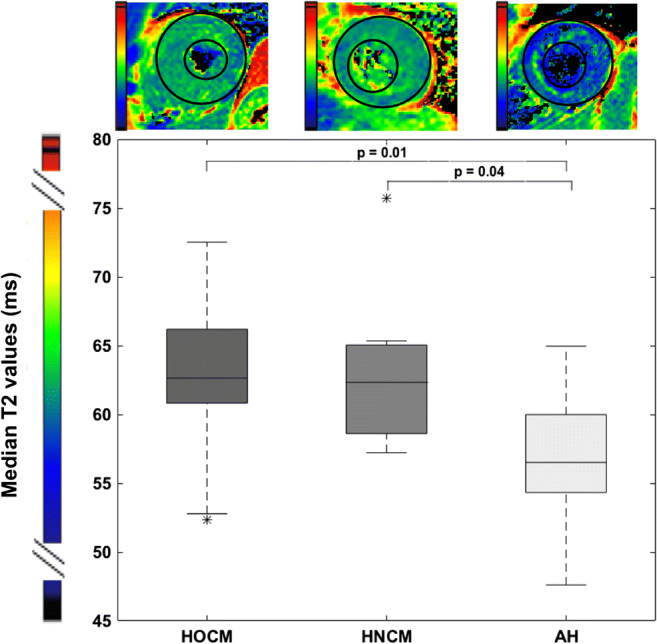
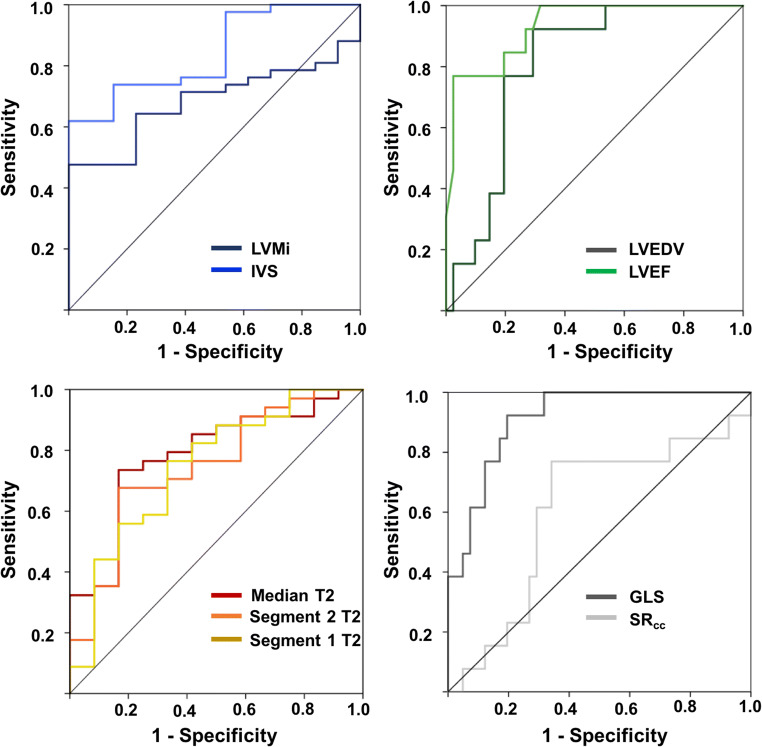
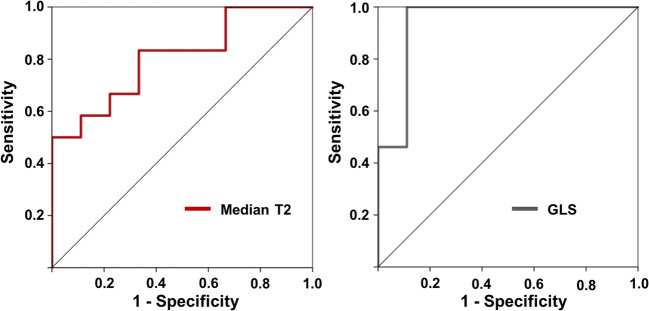
Results: While LVMi was not significantly different, IVS was thickened in HOCM patients compared to athlete's. Absolute values of GLS were significantly increased in patients with HOCM/HNCM compared to AH. Median T2 values were elevated compared to controls except in athlete's heart. ROC analysis revealed T2 values (AUC 0.78) and GLS (AUC 0.91) as good parameters to discriminate AH from overall HNCM/HOCM.
Conclusion: Discrimination of pathologic from non-pathologic LVH has implications for risk assessment of competitive sports in athletes. Multiparametric CMR with parametric T2 mapping and deformation imaging may add information to distinguish AH from LVH due to HCM.
Key points: • Structural analyses using T2 mapping cardiovascular magnetic resonance imaging (CMR) may help to further distinguish myocardial diseases. • To differentiate pathologic from non-pathologic left ventricular hypertrophy, CMR including T2 mapping was obtained in patients with hypertrophic obstructive/non-obstructive cardiomyopathy (HOCM/HNCM) as well as in strength-trained athletes. • Elevated median T2 values in HOCM/HNCM compared with athlete's may add information to distinguish athlete's heart from pathologic left ventricular hypertrophy.
Keywords: Athletes; Cardiomyopathy, hypertrophic; Hypertrophy; Left ventricular; Multiparametric magnetic resonance imaging.
Conflict of interest statement
One of the authors of this manuscript (Bernhard Schnackenburg) is an employee of Philips Healthcare. The remaining authors declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Maron BJ, Shirani J, Poliac LC, Mathenge R, Roberts WC, Mueller FO (1996) Sudden death in young competitive athletes. JAMA 276:199–204. 10.1001/jama.1996.03540030033028 - PubMed
-
- Pelliccia A, Zipes DP, Maron BJ. Bethesda Conference #36 and the European Society of Cardiology Consensus Recommendations Revisited: A Comparison of U.S. and European Criteria for Eligibility and Disqualification of Competitive Athletes With Cardiovascular Abnormalities. J Am Coll Cardiol. 2008;52:1990–1996. doi: 10.1016/j.jacc.2008.08.055. - DOI - PubMed
-
- Cardim N, Galderisi M, Edvardsen T, et al. Role of multimodality cardiac imaging in the management of patients with hypertrophic cardiomyopathy: an expert consensus of the European Association of Cardiovascular Imaging Endorsed by the Saudi Heart Association. Eur Heart J Cardiovasc Imaging. 2015;16:280–280. doi: 10.1093/ehjci/jeu291. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
