

Mus musculus papillomavirus 1 is a key driver of skin cancer development upon immunosuppression
- PMID: 33063442
- PMCID: PMC7894140
- DOI: 10.1111/ajt.16358
Mus musculus papillomavirus 1 is a key driver of skin cancer development upon immunosuppression
Abstract
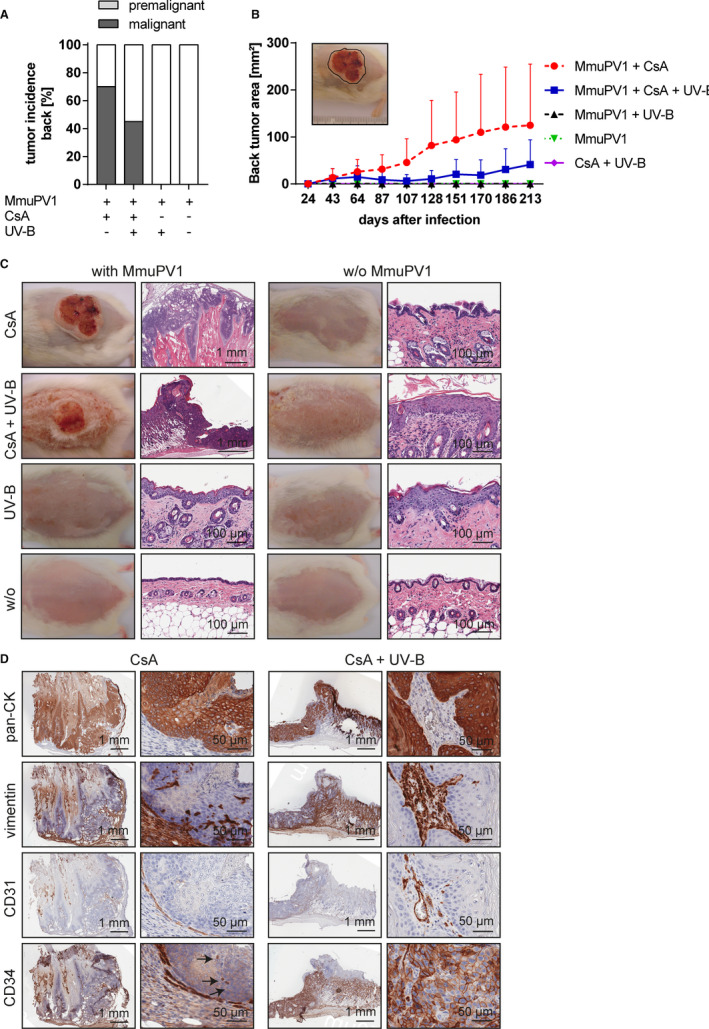
Epidemiological and experimental data implicate cutaneous human papillomavirus infection as co-factor in the development of cutaneous squamous cell carcinomas (cSCCs), particularly in immunocompromised organ transplant recipients (OTRs). Herein, we established and characterized a skin cancer model, in which Mus musculus papillomavirus 1 (MmuPV1) infection caused cSCCs in cyclosporine A (CsA)-treated mice, even in the absence of UV light. Development of cSCCs and their precursors were observed in 70% of MmuPV1-infected, CsA-treated mice on back as well as on tail skin. Immunosuppression by systemic CsA, but not UV-B irradiation, was a prerequisite, as immunocompetent or UV-B-irradiated mice did not develop skin malignancies after infection. In the virus-driven cSCCs the MmuPV1-E6/E7 oncogenes were abundantly expressed, and transcriptional activity and productive infection demonstrated. MmuPV1 infection induced the expression of phosphorylated H2AX, but not degradation of proapoptotic BAK in the cSCCs. Transfer of primary cells, established from a MmuPV1-induced cSCC from back skin, into athymic nude mice gave rise to secondary cSCCs, which lacked viral DNA, demonstrating that maintenance of the malignant phenotype was virus independent. This papillomavirus-induced skin cancer model opens future investigations into viral involvement, pathogenesis, and cancer surveillance, aiming at understanding and controlling the high incidence of skin cancer in OTRs.
Keywords: animal models: murine; basic (laboratory) research / science; cancer / malignancy / neoplasia: skin - nonmelanoma; dermatology; immunosuppressant - calcineurin inhibitor: cyclosporine A (CsA); immunosuppression / immune modulation; infection and infectious agents - viral; infectious disease.
© 2020 The Authors. American Journal of Transplantation published by Wiley Periodicals LLC on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures








References
-
- Karia PS, Han J, Schmults CD. Cutaneous squamous cell carcinoma: estimated incidence of disease, nodal metastasis, and deaths from disease in the United States, 2012. J Am Acad Dermatol. 2013;68(6):957–966. - PubMed
-
- Rogers HW, Weinstock MA, Feldman SR, et al. Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the U.S. population, 2012. JAMA Dermatology. 2015;151(10):1081–1086. - PubMed
-
- Garrett GL, Blanc PD, Boscardin J, et al. Incidence of and risk factors for skin cancer in organ transplant recipients in the United States. JAMA Dermatology. 2017;153(3):296–303. - PubMed
-
- Mudigonda T, Levender MM, O'Neill JL, et al. Incidence, risk factors, and preventative management of skin cancers in organ transplant recipients: a review of single‐ and multicenter retrospective studies from 2006 to 2010. Dermatol Surg. 2013;39(3 Pt 1):345–364. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
