

Perceived Need for Psychosocial Support After Aortic Dissection: Cross-Sectional Survey
- PMID: 33064108
- PMCID: PMC7434062
- DOI: 10.2196/15447
Perceived Need for Psychosocial Support After Aortic Dissection: Cross-Sectional Survey
Abstract
Background: The gold standard management of aortic dissection, a life-threatening condition, includes multidisciplinary approaches. Although mental distress following aortic dissection is common, evidence-based psychosocial interventions for aortic dissection survivors are lacking.
Objective: The aim of this study is to identify the perceived psychosocial needs of aortic dissection survivors by surveying patients, their relatives, and health professionals to inform the development of such interventions.
Methods: This study used a cross-sectional survey and collected responses from 41 participants (27 patients with aortic dissection, 8 relatives of patients with aortic dissection, and 6 health professionals) on key topics, types of interventions, best timing, anticipated success, and the intended effects and side effects of psychosocial interventions after aortic dissection.
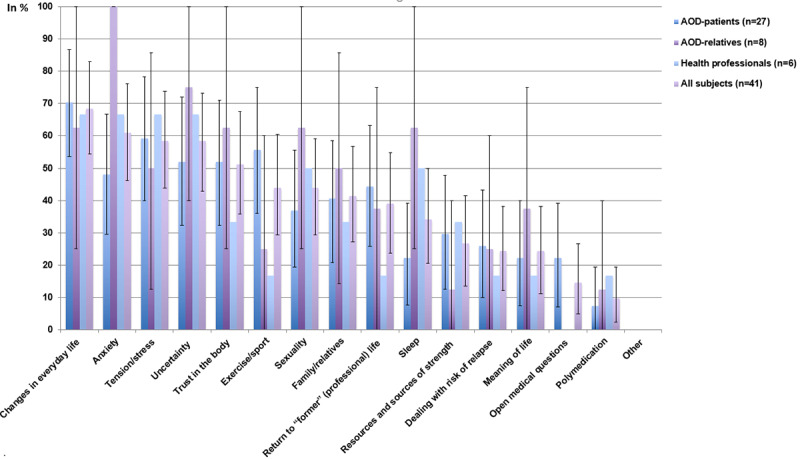
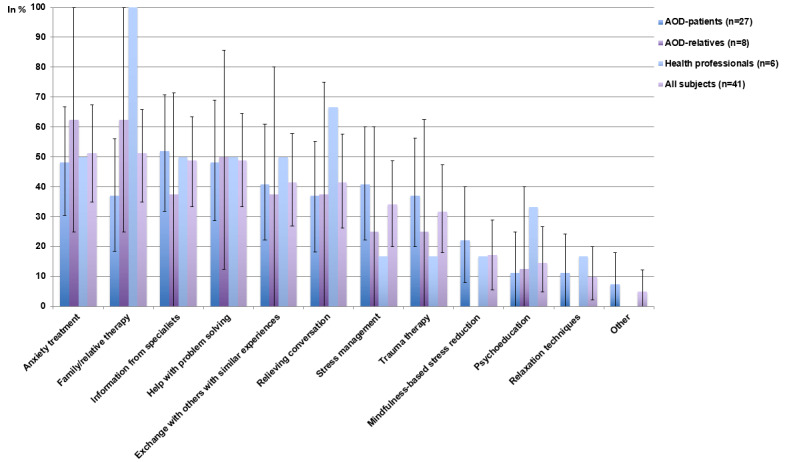
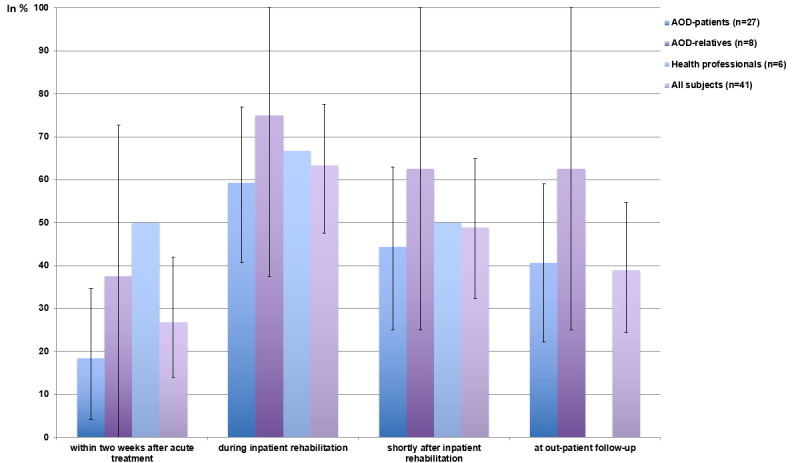
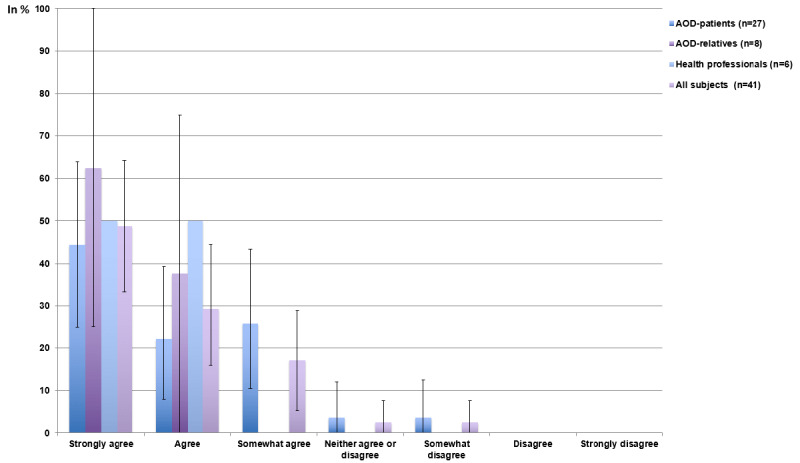
Results: The principal intervention topics were "changes in everyday life" (28/41, 68%, 95% CI 54.5%-82.9%), "anxiety" (25/41, 61%, 95% CI 46.2%-76.2%), "uncertainty" (24/41, 59%, 95% CI 42.9%-73.2%), "tension/distress" (24/41, 59%, 95% CI 43.9%-73.8%), and "trust in the body" (21/41, 51%, 95% CI 35.9%-67.5%). The most commonly indicated intervention types were "family/relative therapy" (21/41, 51%, 95% CI 35%-65.9%) and "anxiety treatment" (21/41, 51%, 95% CI 35%-67.5%). The most recommended intervention timing was "during inpatient rehabilitation" (26/41, 63%, 95% CI 47.6%-77.5%) followed by "shortly after inpatient rehabilitation" (20/41, 49%, 95% CI 32.4%-65%). More than 95% (39/41) of respondents anticipated a benefit from psychosocial interventions following aortic dissection dissection, expecting a probable improvement in 68.6% (95% CI 61.4%-76.2%) of aortic dissection survivors, a worse outcome for 5% (95% CI 2.9%-7.9%), and that 6% (95% CI 1.8%-10.4%) would have negative side effects due to such interventions.
Conclusions: Our findings highlight a substantial need for psychosocial interventions in aortic dissection survivors and indicate that such interventions would be a success. They provide a basis for the development and evaluation of interventions as part of state-of-the-art aortic dissection management.
Keywords: aortic dissection; patient involvement; psychosocial support; psychosomatic; psychotherapy; treatment need.
©Gunther Meinlschmidt, Denis Berdajs, Roger Moser-Starck, Alexander Frick, Sebastian Gross, Ulrich Schurr, Friedrich S Eckstein, Sabina Hunziker, Rainer Schaefert. Originally published in Journal of Participatory Medicine (http://jopm.jmir.org), 06.07.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Psychological comorbidity and health-related quality of life and its association with awareness, utilization, and need for psychosocial support in a cancer register-based sample of long-term breast cancer survivors.J Psychosom Res. 2008 Apr;64(4):383-91. doi: 10.1016/j.jpsychores.2007.12.005. J Psychosom Res. 2008. PMID: 18374737
-
Efficacy and acceptability of psychosocial interventions in asylum seekers and refugees: systematic review and meta-analysis.Epidemiol Psychiatr Sci. 2019 Aug;28(4):376-388. doi: 10.1017/S2045796019000027. Epub 2019 Feb 11. Epidemiol Psychiatr Sci. 2019. PMID: 30739625 Free PMC article.
-
The effectiveness of caregiver psychosocial interventions on the psychosocial wellbeing, physical health and quality of life of stroke family caregivers and their stroke survivors: A systematic review.JBI Libr Syst Rev. 2012;10(12):679-797. doi: 10.11124/jbisrir-2012-66. JBI Libr Syst Rev. 2012. PMID: 27820387
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
-
Getting psychosocial interventions into mental health nursing practice: a survey of skill use and perceived benefits to service users.J Adv Nurs. 2014 Apr;70(4):866-77. doi: 10.1111/jan.12248. Epub 2013 Sep 11. J Adv Nurs. 2014. PMID: 24020885
Cited by
-
Current Understanding of Aortic Dissection.Life (Basel). 2022 Oct 14;12(10):1606. doi: 10.3390/life12101606. Life (Basel). 2022. PMID: 36295040 Free PMC article. Review.
References
-
- Howard DPJ, Banerjee A, Fairhead JF, Perkins J, Silver LE, Rothwell PM, Oxford Vascular Study Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control: 10-year results from the Oxford Vascular Study. Circulation. 2013 May 21;127(20):2031–7. doi: 10.1161/CIRCULATIONAHA.112.000483. http://europepmc.org/abstract/MED/23599348 CIRCULATIONAHA.112.000483 - DOI - PMC - PubMed
-
- Gawinecka J, Schönrath F, von Eckardstein A. Acute aortic dissection: pathogenesis, risk factors and diagnosis. Swiss Med Wkly. 2017;147:w14489. doi: 10.4414/smw.2017.14489. http://doi.emh.ch/10.4414/smw.2017.14489 smw-14489 - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
