

Clinical Trial
doi: 10.1159/000184431.
Use of OKT3 with cyclosporin and steroids for reversal of acute kidney and liver allograft rejection
- PMID: 3306422
- PMCID: PMC2994552
- DOI: 10.1159/000184431
Item in Clipboard
Clinical Trial
Use of OKT3 with cyclosporin and steroids for reversal of acute kidney and liver allograft rejection
Nephron.
1987.
Abstract
OKT3 monoclonal antibody therapy was added to preexisting baseline immunosuppressive treatment with ciclosporin and steroids to treat rejection in 52 recipients of cadaveric livers and 10 recipients of cadaveric kidneys. Rejection was controlled in 75% of patients treated, often after high-dose steroid therapy had failed. Rejection recurred during the 17-month follow-up period, after completion of OKT3, in only 25% of the patients who had responded. The safety and effectiveness of this monoclonal therapy, added to ciclosporin and steroids, has been established in this study.
Figures
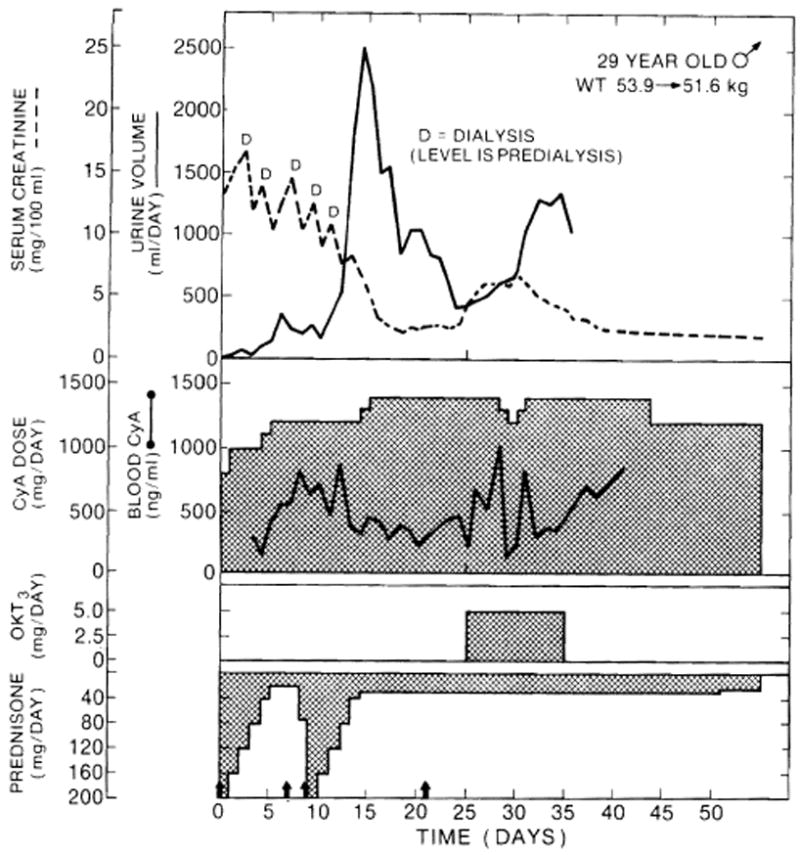
Clinical course of a cadaveric kidney recipient whose graft underwent an initial period of acute tubular necrosis, with a beginning subsequent diuresis that was interrupted by rejection. Arrows: 1 g methylprednisolone. CyA = Ciclosporin.
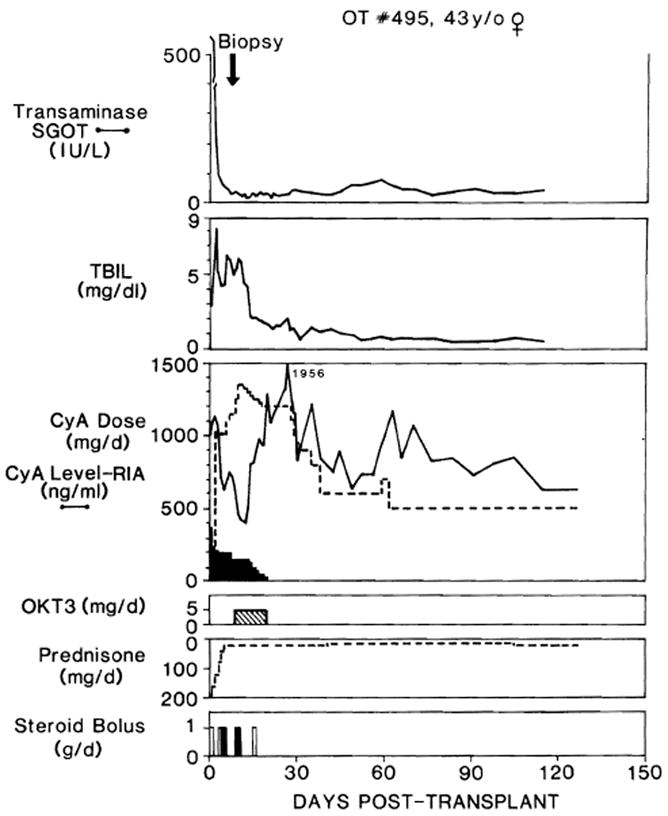
Clinical course of liver recipient OT 495, who developed biopsy-proved rejection after 10 days while undergoing ciclosporin(CyA)-steroid therapy. Note that ciclosporin was given at first by both intravenous (dark shading) and oral (no shading) routes. TBIL = Total bilirubin; SGOT = serum glutamic-oxaloacetic transaminase; steroid bolus: solid bars = methylprednisolone, intravenously; open bars = hydrocortisone intravenously.
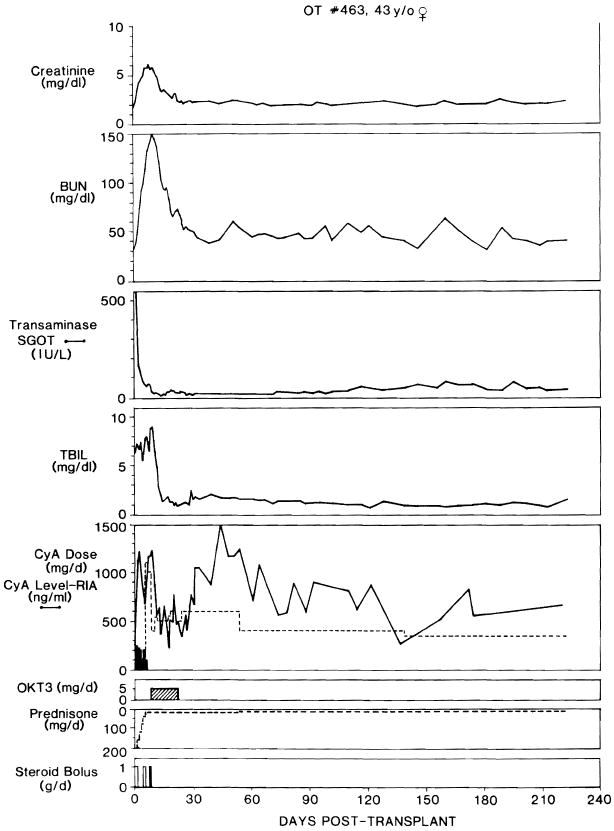
Clinical course of liver recipient OT 463, whose OKT3 course was started after 9 days in part because her renal failure precluded giving therapeutic doses of ciclosporin to treat her presumed rejection. Note resolution of azotemia during OKT3 therapy. Abbreviations and symbols, same as in figure 2.

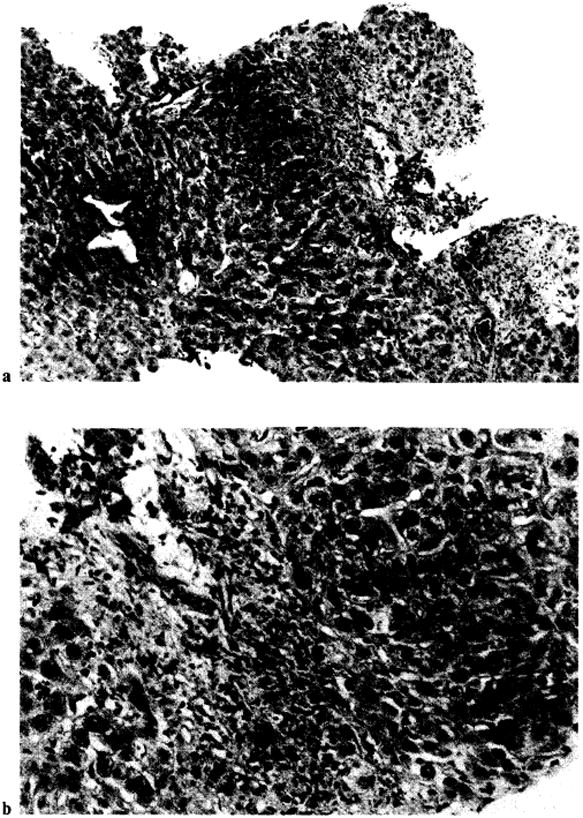
Histologic findings of cellular rejection typical in group 2 liver patients consist of portal mononuclear cell infiltration with damage to bile duct epithelium and endothelium of vessels (arrow). The patient, OT 407, had a repeat biopsy after therapy (fig. 8). a × 125. b × 315.
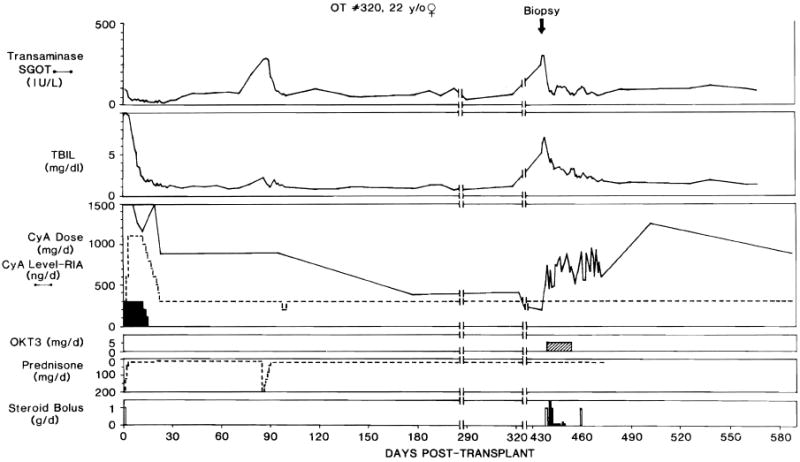
Clinical course ofliver recipient OT 320 treated with OKT3 for acute rejection 14 months after transplantation. Abbreviations and symbols, same as in figure 2.
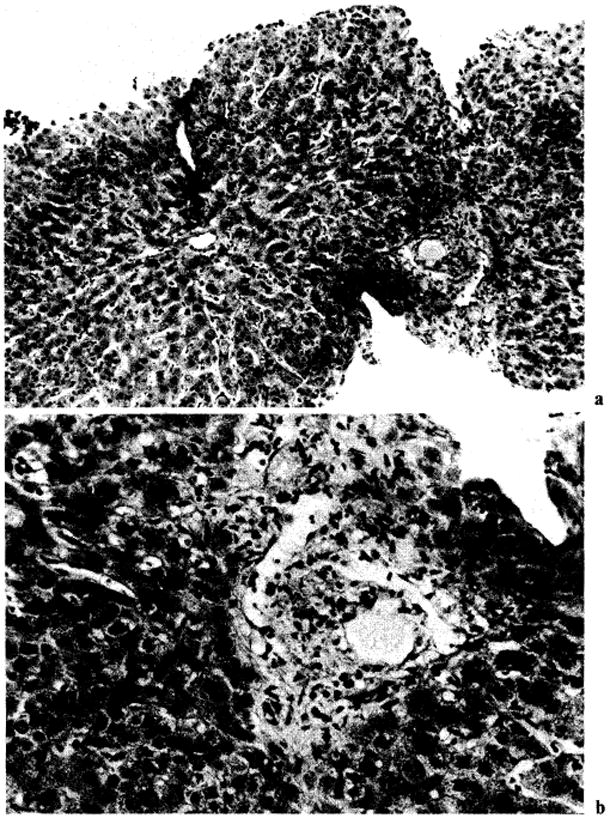
Patient OT 377. Histologic findings of chronic rejection. Note paucity of bile ducts and fibrosis in portal tracts. a × 125. b × 315.
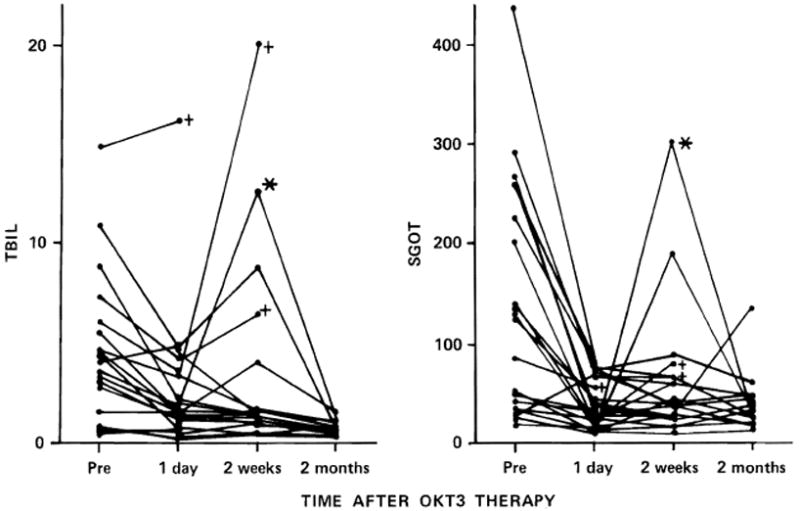
Response of serum bilirubin (TBIL) and serum glutamic oxaloacetic transaminase (SGOT) in the patients of group 2, whose rejection was diagnosed between 10 days and 3 months after liver replacement. The crosses indicate the loss of the graft, and the asterisk is on the curve of a patient who developed herpes virus hepatitis after OKT3 therapy.
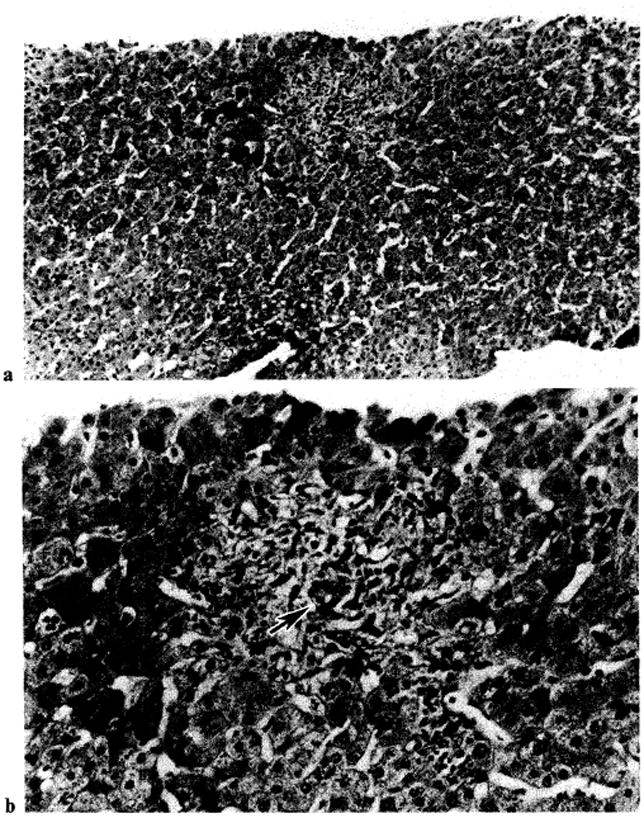
Improvement of histologic findings of liver patient OT 407, whose biopsy before OKT3 therapy is shown in figure 4. Note marked decrease of inflammatory cells after OKT3 therapy and intact bile ductule (arrow). a × 125. b × 315.
Improvement of histologic findings of liver patient OT 377 after OKT3 therapy. The pretreatment biopsy is shown in figure 6. Note reduction of mononuclear cells. However, no bile ductules were seen in this biopsy, and there was an increase in centrilobular canalicular cholestasis. a × 125. b × 315.
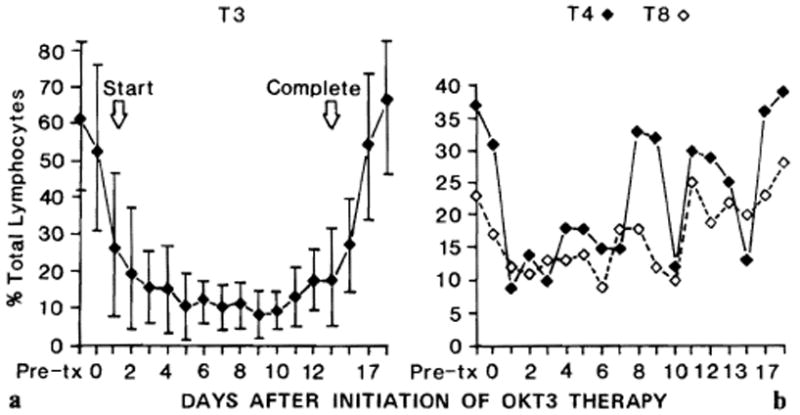
Influence of OKT3 therapy on T-cell subpopulations in liver recipients during rejection. a Percent of total circulating lymphocytes that bear the T3 antigen as determined by direct immunofluorescence (with standard deviations). b Percent of total circulating lymphocytes bearing T4 and T8 by direct immunofluorescence in the same patients as in a. Average number of observations per data point was 10.
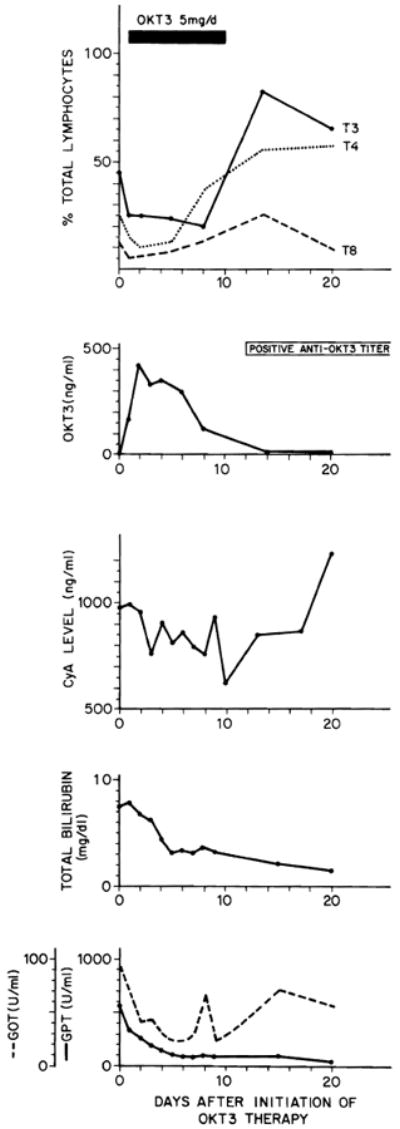
Events in patient OT 469, whose biopsy-proved rejection was reversed with OKT3 therapy. Treatment was started on the 6th postoperative day. Note the persistence of T3-positive lymphocytes in the circulation and T3 modulation during OKT3 therapy as well as the lymphocyte rebound after discontinuance of therapy. CyA = Ciclosporin. GOT = glutamic oxaloacetic transaminase; GPT = glutamic pyruvate transaminase.
References
-
- Griepp R, Stinson E, Dong E, et al. The use of antithymocyte globulin in human heart transplantation. Circulation. 1972;45(suppl 1):147–153. - PubMed
-
- Glass N, Miller D, Sollinger H, et al. A comparative study of steroid and heterologous antiserum in the treatment of acute renal allograft rejection. Transplant Proc. 1983;15:617–621.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources