

Epidemiology, clinical characteristics, and outcome of candidemia in critically ill patients in Germany: a single-center retrospective 10-year analysis
- PMID: 33064220
- PMCID: PMC7567770
- DOI: 10.1186/s13613-020-00755-8
Epidemiology, clinical characteristics, and outcome of candidemia in critically ill patients in Germany: a single-center retrospective 10-year analysis
Abstract
Background: Despite advances in the management of bloodstream infections (BSI) caused by Candida spp., the mortality still remains high in critically ill patients. The worldwide epidemiology of yeast-related BSI is subject to changing species distribution and resistance patterns, challenging antifungal treatment strategies. The aim of this single-center study was to identify predictors of mortality after 28 and 180 days in a cohort of mixed surgical and medical critically ill patients with candidemia.
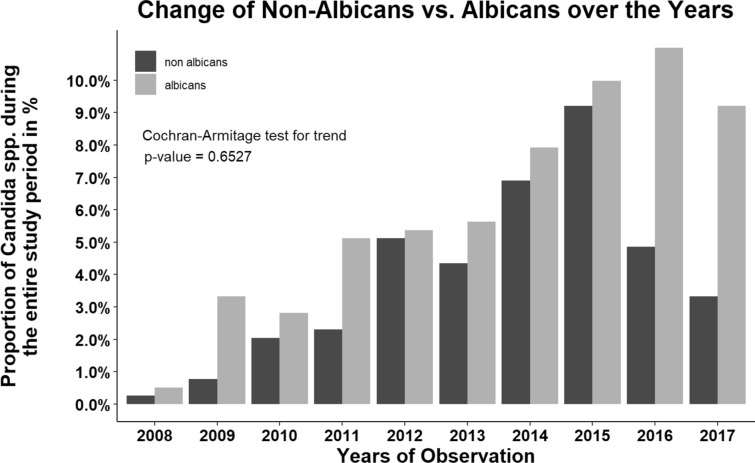
Methods: Patients, who had been treated for laboratory-confirmed BSI caused by Candida spp. in one of 12 intensive care units (ICU) at a University hospital between 2008 and 2017, were retrospectively identified. We retrieved data including clinical characteristics, Candida species distribution, and antifungal management from electronic health records to identify risk factors for mortality at 28 and 180 days using a Cox regression model.
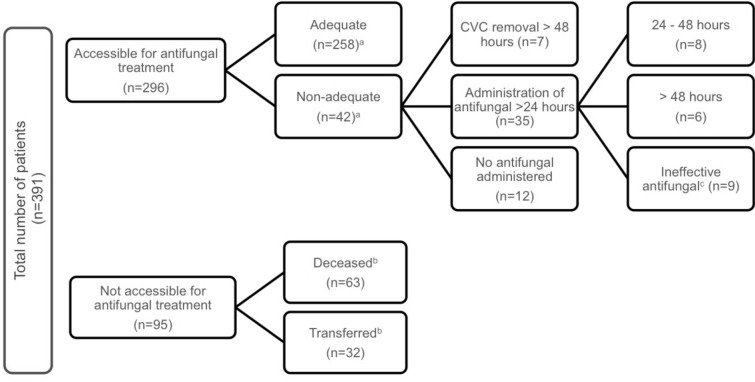
Results: A total of 391 patients had blood cultures positive for Candida spp. (incidence 4.8/1000 ICU admissions). The mortality rate after 28 days was 47% (n = 185) and increased to 60% (n = 234) after 180 days. Age (HR 1.02 [95% CI 1.01-1.03]), a history of liver cirrhosis (HR 1.54 [95% CI 1.07-2.20]), septic shock (HR 2.41 [95% CI 1.73-3.37]), the Sepsis-related Organ Failure Assessment score (HR 1.12 [95% CI 1.07-1.17]), Candida score (HR 1.25 [95% CI 1.11-1.40]), and the length of ICU stay at culture positivity (HR 1.01 [95% CI 1.00-1.01]) were significant risk factors for death at 180 days. Patients, who had abdominal surgery (HR 0.66 [95% CI 0.48-0.91]) and patients, who received adequate (HR 0.36 [95% CI 0.24-0.52]) or non-adequate (HR 0.31 [95% CI 0.16-0.62]) antifungal treatment, had a reduced mortality risk compared to medical admission and no antifungal treatment, respectively.
Conclusions: The mortality of critically ill patients with Candida BSI is high and is mainly determined by disease severity, multiorgan dysfunction, and antifungal management rather than species distribution and susceptibility. Our results underline the importance of timely treatment of candidemia. However, controversies remain on the optimal definition of adequate antifungal management.
Keywords: Antifungal agents; Bloodstream infection; Candida species; Candidemia; Critically ill patients; Echinocandin; Fluconazole; Intensive care unit.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Ghanem-Zoubi N, Zorbavel D, Khoury J, Geffen Y, Qasum M, Predescu S, et al. The association between treatment appropriateness according to EUCAST and CLSI breakpoints and mortality among patients with candidemia: a retrospective observational study. Eur J Clin Microbiol Infect Dis. 2018;37(12):2397–2404. doi: 10.1007/s10096-018-3389-1. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
