

Palliative Care in High-Grade Glioma: A Review
- PMID: 33066030
- PMCID: PMC7599762
- DOI: 10.3390/brainsci10100723
Palliative Care in High-Grade Glioma: A Review
Abstract
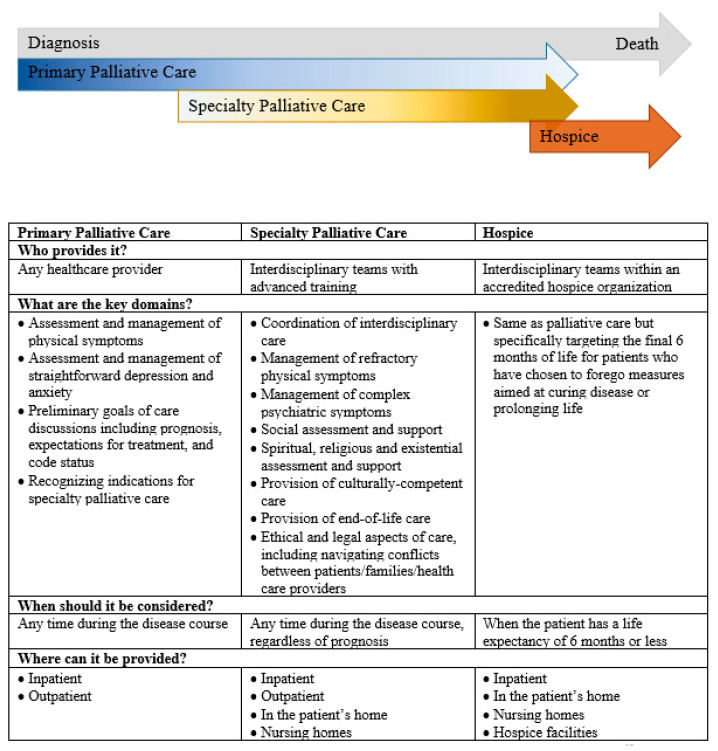
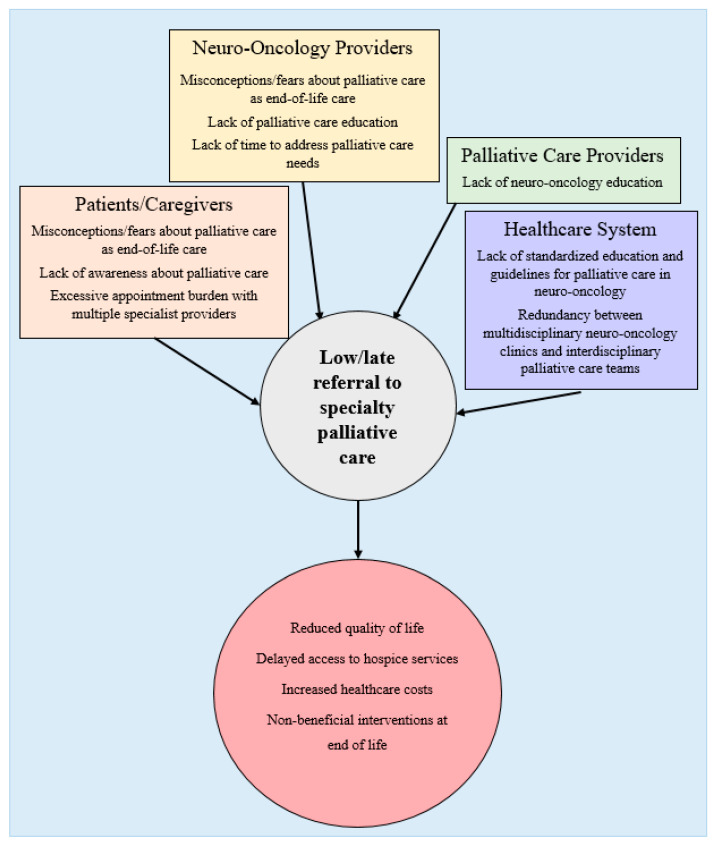
High-grade glioma (HGG) is characterized by debilitating neurologic symptoms and poor prognosis. Some of the suffering this disease engenders may be ameliorated through palliative care, which improves quality of life for seriously ill patients by optimizing symptom management and psychosocial support, which can be delivered concurrently with cancer-directed treatments. In this article, we review palliative care needs associated with HGG and identify opportunities for primary and specialty palliative care interventions. Patients with HGG and their caregivers experience high levels of distress due to physical, emotional, and cognitive symptoms that negatively impact quality of life and functional independence, all in the context of limited life expectancy. However, patients typically have limited contact with specialty palliative care until the end of life, and there is no established model for ensuring their palliative care needs are met throughout the disease course. We identify low rates of advance care planning, misconceptions about palliative care being synonymous with end-of-life care, and the unique neurologic needs of this patient population as some of the potential barriers to increased palliative interventions. Further research is needed to define the optimal roles of neuro-oncologists and palliative care specialists in the management of this illness and to establish appropriate timing and models for palliative care delivery.
Keywords: glioma; palliative care; quality of life; supportive care.
Conflict of interest statement
The authors report no conflict of interest. Diamond discloses nonfinancial support from Third Rock Ventures, outside the submitted work.
Figures
References
-
- Cancer Facts & Figures. American Cancer Society. [(accessed on 17 January 2020)];2019 Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-....
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
