

Ticagrelor monotherapy in patients with concomitant diabetes mellitus and chronic kidney disease: a post hoc analysis of the GLOBAL LEADERS trial
- PMID: 33066794
- PMCID: PMC7568378
- DOI: 10.1186/s12933-020-01153-x
Ticagrelor monotherapy in patients with concomitant diabetes mellitus and chronic kidney disease: a post hoc analysis of the GLOBAL LEADERS trial
Abstract
Background: Patients with both diabetes mellitus (DM) and chronic kidney disease (CKD) are a subpopulation characterized by ultrahigh ischemic and bleeding risk after percutaneous coronary intervention. There are limited data on the impact of ticagrelor monotherapy among these patients.
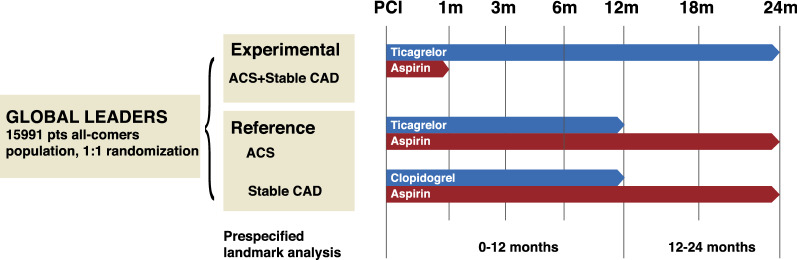
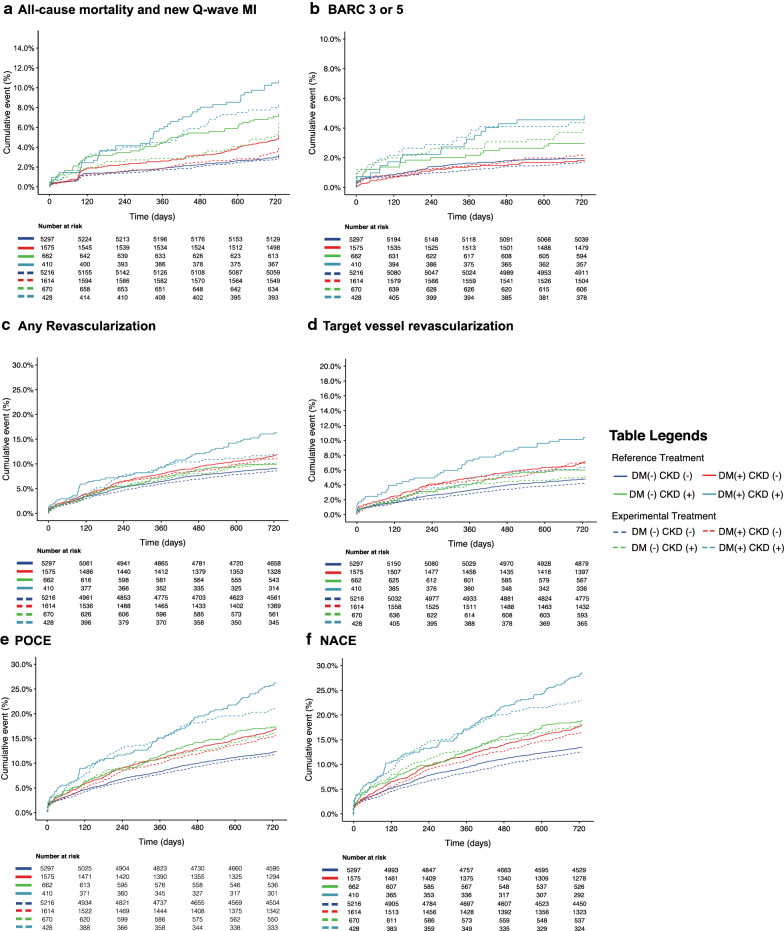
Methods: In this post hoc analysis of the GLOBAL-LEADERS trial, the treatment effects of the experimental (one-month dual-antiplatelet therapy [DAPT] followed by 23-month ticagrelor monotherapy) versus the reference regimen (12-month DAPT followed by 12-month aspirin alone) were analyzed according to DM/CKD status. The primary endpoint was a composite endpoint of all-cause death or new Q-wave myocardial infarction at 2-years. The patient-oriented composite endpoint (POCE) was defined as the composite of all-cause death, any stroke, site-reported MI and any revascularization, whereas net adverse clinical events (NACE) combined POCE with BARC type 3 or 5 bleeding events.
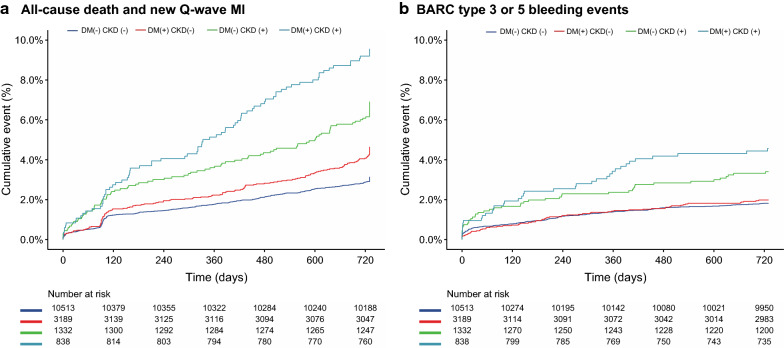
Results: At 2 years, the DM + /CKD + patients had significantly higher incidences of the primary endpoint (9.5% versus 3.1%, adjusted HR 2.16; 95% CI [1.66-2.80], p < 0.001), BARC type 3 or 5 bleeding events, stroke, site-reported myocardial infraction, all revascularization, POCE, and NACE, compared with the DM-/CKD- patients. Among the DM + /CKD + patients, after adjustment, there were no significant differences in the primary endpoints between the experimental and reference regimen; however, the experimental regimen was associated with lower rates of POCE (20.6% versus 25.9%, HR 0.74; 95% CI [0.55-0.99], p = 0.043, pinteraction = 0.155) and NACE (22.7% versus 28.3%, HR 0.75; 95% CI [0.56-0.99], p = 0.044, pinteraction = 0.310), which was mainly driven by a lower rate of all revascularization, as compared with the reference regimen. The landmark analysis showed that while the experimental and reference regimen had similar rates of all the clinical endpoints during the first year, the experimental regimen was associated with significantly lower rates of POCE (5.8% versus 11.0%, HR 0.49; 95% CI [0.29-0.82], p = 0.007, pinteraction = 0.040) and NACE (5.8% versus 11.2%, HR 0.48; 95% CI [0.29-0.82], p = 0.007, pinteraction = 0.013) in the second year.
Conclusion: Among patients with both DM and CKD, ticagrelor monotherapy was not associated with lower rates of all-cause death or new Q-wave, or major bleeding complications; however, it was associated with lower rates of POCE and NACE. These findings should be interpreted as hypothesis-generating.
Clinical trial registration: ClinicalTrials.gov (NCT01813435).
Keywords: Aspirin-free antiplatelet strategies; Chronic kidney disease; DAPT; Diabetes mellitus; Percutaneous coronary intervention; Ticagrelor.
Conflict of interest statement
Dr. Steg received grants and personal fees from Bayer/Janssen, grants and personal fees from Merck, grants and personal fees from Sanofi, grants and personal fees from Amarin, personal fees from Amgen, personal fees from Bristol Myers Squibb, personal fees from Boehringer-Ingelheim, personal fees from Pfizer, personal fees from Novartis, personal fees from Regeneron, personal fees from Lilly, personal fees from AstraZeneca, grants, personal fees and non-financial support from Servier, outside the submitted work. Dr. Hamm received advisory Board fees from AstraZeneca. Dr. van Geuns received speakers fee from Abbott Vascular and Boston Scientific. Dr. Onuma reports being a member of advisory board of Abbott vascular. Dr. Serruys reports personal fees from Biosensors, personal fees from Cardialysis, personal fees from Medtronic, personal fees from Micel Technologies, personal fees from Sinomedical Sciences Technology, personal fees from Philips/Volcano, personal fees from Xeltis, personal fees from HeartFlow, outside the submitted work. Dr. Angiolillo has received payment as an individual for: reports receiving payments as an individual for: a) Consulting fee or honorarium from Amgen, Aralez, AstraZeneca, Bayer, Biosensors, Boehringer Ingelheim, Bristol-Myers Squibb, Chiesi, Daiichi-Sankyo, Eli Lilly, Haemonetics, Janssen, Merck, PhaseBio, PLx Pharma, Pfizer, Sanofi, and The Medicines Company; b) Participation in review activities from CeloNova and St. Jude Medical. Institutional payments for grants from Amgen, AstraZeneca, Bayer, Biosensors, CeloNova, CSL Behring, Daiichi-Sankyo, Eisai, Eli-Lilly, Gilead, Idorsia, Janssen, Matsutani Chemical Industry Co., Merck, Novartis, Osprey Medical, and Renal Guard Solutions.
Figures
References
-
- Franchi F, Rollini F, Angiolillo DJ. Defining the link between chronic kidney disease, high platelet reactivity, and clinical outcomes in clopidogrel-treated patients undergoing percutaneous coronary intervention. Circ Cardiovasc Interv. 2015;8(6):e002760. doi: 10.1161/CIRCINTERVENTIONS.115.002760. - DOI - PubMed
-
- Baber U, Farkouh ME, Arbel Y, Muntner P, Dangas G, Mack MJ, Hamza TH, Mehran R, Fuster V. Comparative efficacy of coronary artery bypass surgery vs percutaneous coronary intervention in patients with diabetes and multivessel coronary artery disease with or without chronic kidney disease. Eur Heart J. 2016;37(46):3440–3447. doi: 10.1093/eurheartj/ehw378. - DOI - PubMed
