

The healthy exocrine pancreas contains preproinsulin-specific CD8 T cells that attack islets in type 1 diabetes
- PMID: 33067232
- PMCID: PMC7567597
- DOI: 10.1126/sciadv.abc5586
The healthy exocrine pancreas contains preproinsulin-specific CD8 T cells that attack islets in type 1 diabetes
Abstract
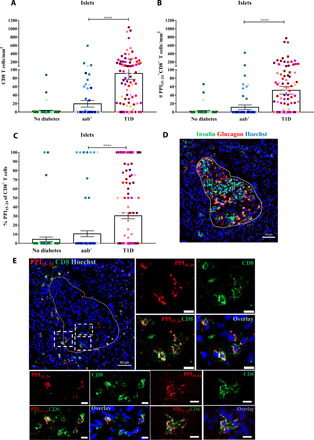
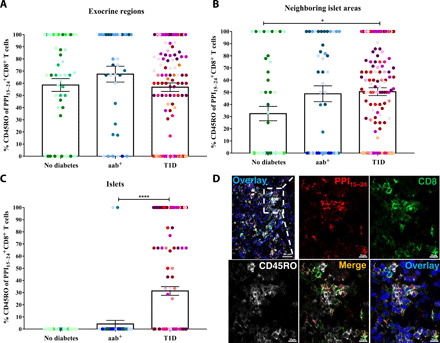
Preproinsulin (PPI) is presumably a crucial islet autoantigen found in patients with type 1 diabetes (T1D) but is also recognized by CD8+ T cells from healthy individuals. We quantified PPI-specific CD8+ T cells within different areas of the human pancreas from nondiabetic controls, autoantibody-positive donors, and donors with T1D to investigate their role in diabetes development. This spatial cellular quantitation revealed unusually high frequencies of autoreactive CD8+ T cells supporting the hypothesis that PPI is indeed a key autoantigen. To our surprise, PPI-specific CD8+ T cells were already abundantly present in the nondiabetic pancreas, thus questioning the dogma that T1D is caused by defective thymic deletion or systemic immune dysregulation. During T1D development, these cells accumulated in and around islets, indicating that an islet-specific trigger such as up-regulation of major histocompatibility complex class I might be essential to unmask beta cells to the immune system.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. Distributed under a Creative Commons Attribution NonCommercial License 4.0 (CC BY-NC).
Figures



References
-
- Katsarou A., Gudbjörnsdottir S., Rawshani A., Dabelea D., Bonifacio E., Anderson B. J., Jacobsen L. M., Schatz D. A., Lernmark Å., Type 1 diabetes mellitus. Nat. Rev. Dis. Primers. 3, 17016 (2017). - PubMed
-
- Babon J. A. B., De Nicola M. E., Blodgett D. M., Crèvecoeur I., Buttrick T. S., Maehr R., Bottino R., Naji A., Kaddis J., Elyaman W., James E. A., Haliyur R., Brissova M., Overbergh L., Mathieu C., Delong T., Haskins K., Pugliese A., Campbell-Thompson M., Mathews C., Atkinson M. A., Powers A. C., Harlan D. M., Kent S. C., Analysis of self-antigen specificity of islet-infiltrating T cells from human donors with type 1 diabetes. Nat. Med. 22, 1482–1487 (2016). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
