

Prevalence and factors associated with multidrug-resistant tuberculosis in South India
- PMID: 33067551
- PMCID: PMC7567814
- DOI: 10.1038/s41598-020-74432-y
Prevalence and factors associated with multidrug-resistant tuberculosis in South India
Abstract
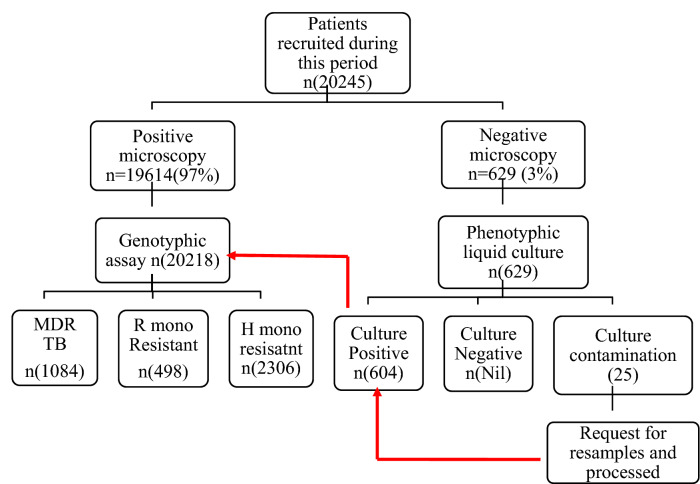
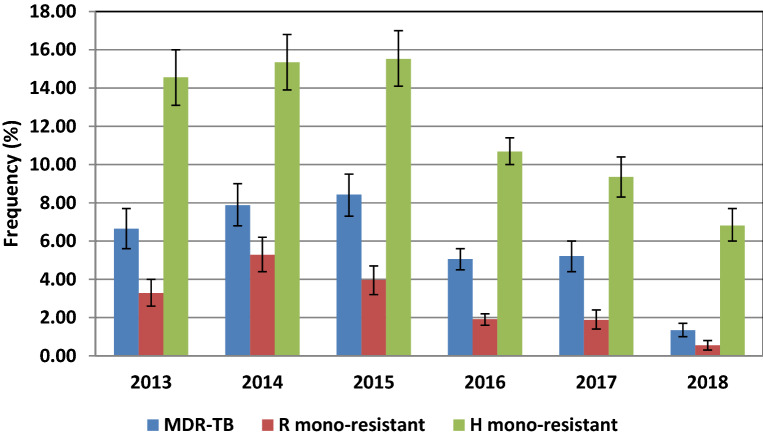
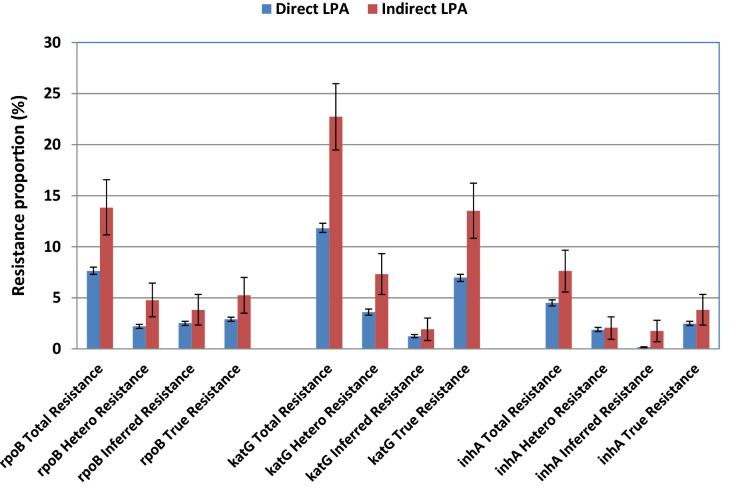
India accounts for about one-fourth of the global burden of MDR-TB. This study aims to assess the prevalence and factors associated with tuberculosis drug resistance among patients from South India. MTBDRplus assay and MGIT liquid culture performed on 20,245 sputum specimens obtained from presumptive MDR-TB cases during a six-year period from 2013 to 2018 were analyzed retrospectively. Univariate and multivariate logistic regression analysis was carried out to evaluate factors associated with MDR, Rifampicin mono-resistance, and Isoniazid mono-resistance. MDR, Rifampicin mono- resistant and Isoniazid mono-resistant TB were found in 5.4%, 2.5%, and 11.4% cases of presumptive MDR-TB, respectively. Based on the rpoB gene, true resistance, hetero-resistance, and inferred resistance to Rifampicin was found in 38%, 29.3%, and 32.7% of the 1582 MDR cases, respectively. S450L (MUT3) was the most common rpoB mutation present in 59.4% of the Rifampicin resistant cases. Of the 3390 Isoniazid resistant cases, 72.5% had mutations in the katG gene, and 27.5% had mutations in the inhA gene. True resistance, heteroresistance, and inferred resistance accounted for 42.9%, 22.2%, and 17.3% of the 2459 katG resistant cases, respectively. True resistance, heteroresistance, and inferred resistance for the inhA gene were found in 54.5%, 40.7%, and 4.7% cases, respectively. MDR-contact (AOR 3.171 95% CI: 1.747-5.754, p-0.000) treatment failure (AOR 2.17595% CI: 1.703-2.777, p-0.000) and female gender (AOR 1.315 95% CI: 1.117-1.548, p-0.001), were positively associated with MDR-TB. Previous TB treatment did not show a significant positive association with MDR (AOR 1.113 95% CI: 0.801-1.546, p-0.523). Old age (AOR 0.994 95% CI: 0.990-0.999, p-0.023) and HIV seropositivity (AOR 0.580 95% CI: 0.369-0.911, p-0.018) were negatively associated with MDR-TB. Although Rifampicin mono-resistance had a positive association with treatment failure (AOR 2.509 95% CI: 1.804-3.490, p < .001), it did not show any association with previous TB treatment (AOR 1.286 95% CI: 0.765-2.164, p-0.342) or with history of contact with MDR-TB (AOR 1.813 95% CI: 0.591-5.560, p-0.298). However, INH mono-resistance showed a small positive association with the previous history of treatment for TB (AOR 1.303 95% CI: 1.021-1.662, p-0.033). It was also positively associated (AOR 2.094 95% CI: 1.236-3.548, p-0.006) with MDR-TB contacts. Thus INH resistance may develop during treatment if compliance has not adhered too and may be easily passed on to the contacts while Rifampicin resistance is probably due to factors other than treatment compliance. MDR-TB, i.e. resistance to both Rifampicin and Isoniazid, is strongly correlated with treatment failure, spread through contact, and not to treatment compliance. The temporal trend in this region shows a decrease in MDR prevalence from 8.4% in 2015 to 1.3% in 2018. A similar trend is observed for Rifampicin mono-resistance and Isoniazid mono-resistance, pointing to the effectiveness of the TB control program. The higher proportion of inferred resistance observed for Rifampicin compared with INH may indicate a surfeit of mechanisms that enable rifampicin resistance. Association of MDR-TB with age, gender, and HIV status suggest the role of the immune system in the emergence of the MDR phenotype.
Conflict of interest statement
The authors declare no competing interests
Figures
Similar articles
-
Diagnostic accuracy and usefulness of the Genotype MTBDRplus assay in diagnosing multidrug-resistant tuberculosis in Cameroon? a cross-sectional study.BMC Infect Dis. 2017 May 31;17(1):379. doi: 10.1186/s12879-017-2489-3. BMC Infect Dis. 2017. PMID: 28569148 Free PMC article.
-
Comparative evaluation of GenoType MTBDRplus line probe assay with solid culture method in early diagnosis of multidrug resistant tuberculosis (MDR-TB) at a tertiary care centre in India.PLoS One. 2013 Sep 5;8(9):e72036. doi: 10.1371/journal.pone.0072036. eCollection 2013. PLoS One. 2013. PMID: 24039735 Free PMC article.
-
Profile of drug-resistant-conferring mutations among new and previously treated pulmonary tuberculosis cases from Aligarh region of Northern India.Int J Mycobacteriol. 2018 Oct-Dec;7(4):315-327. doi: 10.4103/ijmy.ijmy_98_18. Int J Mycobacteriol. 2018. PMID: 30531028
-
Poor treatment outcome and associated risk factors among patients with isoniazid mono-resistant tuberculosis: A systematic review and meta-analysis.PLoS One. 2023 Jul 19;18(7):e0286194. doi: 10.1371/journal.pone.0286194. eCollection 2023. PLoS One. 2023. PMID: 37467275 Free PMC article.
-
Multidrug-resistant tuberculosis.Clin Chim Acta. 2024 Jun 1;559:119701. doi: 10.1016/j.cca.2024.119701. Epub 2024 May 1. Clin Chim Acta. 2024. PMID: 38697459 Review.
Cited by
-
Double trouble: compounding effects of COVID-19 pandemic and antimicrobial resistance on drug resistant TB epidemiology in India.Front Public Health. 2023 Dec 6;11:1305655. doi: 10.3389/fpubh.2023.1305655. eCollection 2023. Front Public Health. 2023. PMID: 38125850 Free PMC article. No abstract available.
-
Expanding the Tuberculosis Cascade of Care to Treat Undiagnosed and Subclinical Tuberculosis in High-Burden Settings.Am J Respir Crit Care Med. 2022 Jan 15;205(2):149-151. doi: 10.1164/rccm.202111-2528ED. Am J Respir Crit Care Med. 2022. PMID: 34818134 Free PMC article. No abstract available.
-
Impact of alcohol drinking and tobacco smoking on the drug-resistance of newly diagnosed tuberculosis: a retrospective cohort study in Shandong, China, during 2004-2020.BMJ Open. 2022 Jul 28;12(7):e059149. doi: 10.1136/bmjopen-2021-059149. BMJ Open. 2022. PMID: 35902191 Free PMC article.
-
Epidemiology of first- and second-line drugs-resistant pulmonary tuberculosis in Iran: Systematic review and meta-analysis.J Clin Tuberc Other Mycobact Dis. 2024 Mar 16;35:100430. doi: 10.1016/j.jctube.2024.100430. eCollection 2024 May. J Clin Tuberc Other Mycobact Dis. 2024. PMID: 38560029 Free PMC article. Review.
-
Extra-long treatment of MDR-TB osteomyelitis of humerus due to neurotoxicity from the 2nd-line drugs: a case report.Egypt J Intern Med. 2023;35(1):41. doi: 10.1186/s43162-023-00225-0. Epub 2023 Jun 13. Egypt J Intern Med. 2023. PMID: 37333427 Free PMC article.
References
-
- World Health Organization (2018) Geneva, Switzerland: WHO; 2018. Global tuberculosis report.
-
- World Health Organization (2019) Geneva, Switzerland: WHO; 2019. Global tuberculosis report.
-
- World Health Organization . Molecular line probe assay for rapid screening ofpatients at risk of multidrug-resistant tuberculosis (MDRTB) Geneva: WorldHealth Organization; 2008.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
