

A multi-country study of prevalence and early childhood mortality among children with omphalocele
- PMID: 33067932
- PMCID: PMC7722785
- DOI: 10.1002/bdr2.1822
A multi-country study of prevalence and early childhood mortality among children with omphalocele
Abstract
Background: Omphalocele is the second most common abdominal birth defect and often occurs with other structural and genetic defects. The objective of this study was to determine omphalocele prevalence, time trends, and mortality during early childhood, by geographical region, and the presence of associated anomalies.
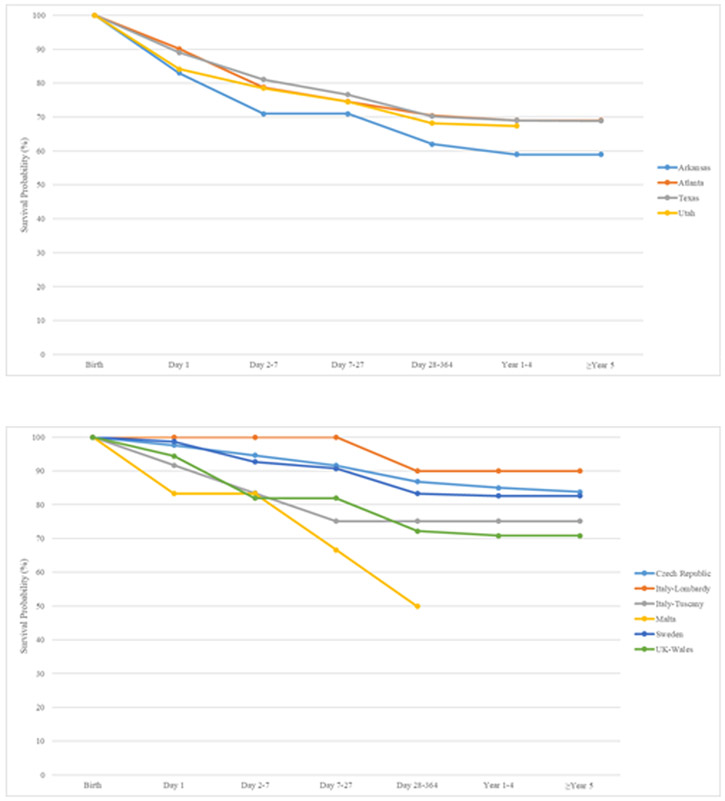
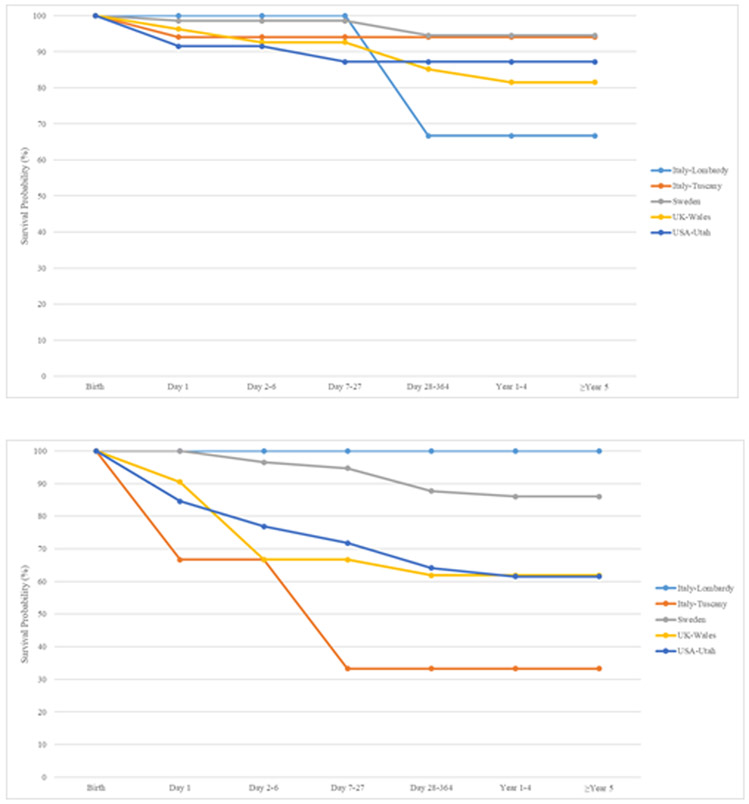
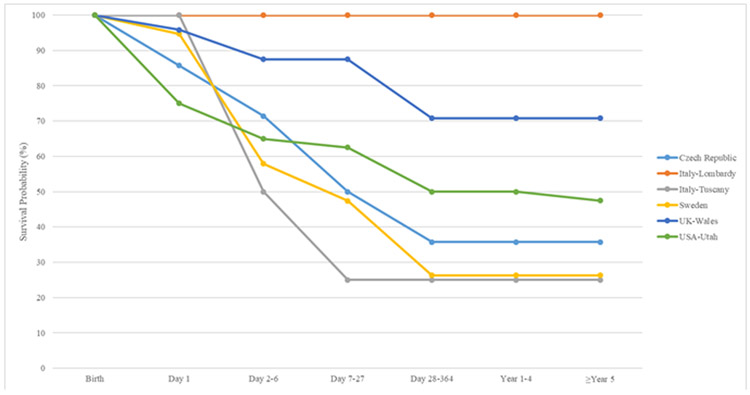
Methods: We conducted a retrospective study with 23 birth defect surveillance systems in 18 countries who are members of the International Clearinghouse for Birth Defects Surveillance and Research that submitted data on cases ascertained from 2000 through 2012, approximately 16 million pregnancies were surveyed that resulted in live births, stillbirths, or elective terminations of pregnancy for fetal anomalies (ETOPFA) and cases with omphalocele were included. Overall prevalence and mortality rates for specific ages were calculated (day of birth, neonatal, infant, and early childhood). We used Kaplan-Meier estimates with 95% confidence intervals (CI) to calculate cumulative mortality and joinpoint regression for time trend analyses.
Results: The prevalence of omphalocele was 2.6 per 10,000 births (95% CI: 2.5, 2.7) and showed no temporal change from 2000-2012 (average annual percent change = -0.19%, p = .52). The overall mortality rate was 32.1% (95% CI: 30.2, 34.0). Most deaths occurred during the neonatal period and among children with multiple anomalies or syndromic omphalocele. Prevalence and mortality varied by registry type (e.g., hospital- vs. population-based) and inclusion or exclusion of ETOPFA.
Conclusions: The prevalence of omphalocele showed no temporal change from 2000-2012. Approximately one-third of children with omphalocele did not survive early childhood with most deaths occurring in the neonatal period.
Keywords: mortality; omphalocele; prevalence; registry; surveillance.
© 2020 Wiley Periodicals LLC.
Figures
References
-
- Parker SE, Mai CT, Canfield MA, et al. Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol. 2010;88(12):1008–1016. - PubMed
-
- Bryon-Scott R, Haan E, Chan A, Bower C, Scott H, Clark K. A population-based study of abdominal wall defects in South Australia and Western Australia. Paediatric and Perinatal Epidemiology. 1998;12:136–151. - PubMed
-
- Forrester MB, Merz RD. Epidemiology of abdominal wall defects, Hawaii, 1986-1997. Teratology. 1999;60(3):117–123. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
