

Immune Therapy, or Antiviral Therapy, or Both for COVID-19: A Systematic Review
- PMID: 33068263
- PMCID: PMC7568461
- DOI: 10.1007/s40265-020-01421-w
Immune Therapy, or Antiviral Therapy, or Both for COVID-19: A Systematic Review
Abstract
Background: Based on current evidence, recent guidelines of the National Institute of Health, USA indicated the use of remdesivir and dexamethasone for the treatment of COVID-19 patients with mild-moderate disease, not requiring high-flow oxygen. No therapeutic agent directed against the immunologic pathogenic mechanisms related to the cytokine release syndrome complicating the disease was indicated.
Objectives: The purpose of this review was to assess the clinical impact of different therapies for COVID-19; thus, helping to identify the optimal management of the disease. To explain the rationale for the different therapeutic approaches, the characteristics of SARS-CoV-2, the pathogenesis of COVID-19, and the immune response triggered by SARS-CoV-2 infection were reported.
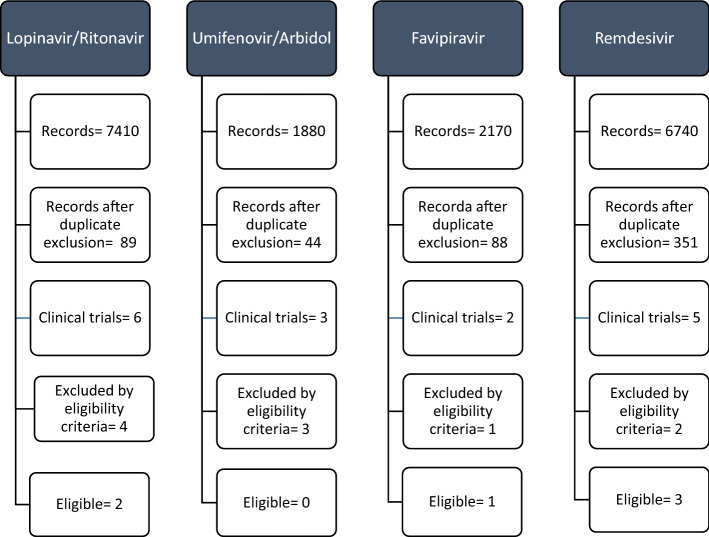
Methods: The efficacy assessment of the different treatments was performed by a systematic review in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Available English language published articles including randomised controlled trials, open-label trials of antivirals and immune therapies extracted from Medline, Google Scholar, and MedRxiv databases were analysed. For inclusion, the primary end point of the trials had to be the efficacy as measured by the improvement of clinical features, or mortality, or the Intensive Care Unit Admission rate, or the discharge number. Case reports, paediatric studies, and studies without control group were excluded. The literature search was extended up to August 15, 2020.
Results: After the removal of duplicate articles, and the exclusion of studies not meeting the eligibility criteria, 2 trials of lopinavir/ritonavir, 1 of favipiravir, 3 of remdesivir, 1 of dexamethasone, 3 of hydroxychloroquine, 2 of colchicine, 6 of tocilizumab, 1 of sarilumab, 1 of siltuximab, 2 of anakinra, 3 of baricitinib, 1 of ruxolitinib, 1 of mavrilimumab, and 1 of itolizumab were suitable for the review. Among antivirals, only remdesivir significantly reduced the time to recovery, and mortality. Data for chloroquine and hydroxychloroquine were largely inconclusive. In a large trial, dexamethasone 6 mg/day reduced mortality by one-third. Trials of tocilizumab and sarilumab did not definitively demonstrate efficacy. Anakinra significantly reduced the mortality in 2 trials. Three retrospective trials on a cumulative number of 145 patients, reported the efficacy of baricitinib, with significant reduction of intensive care unit admission, and deaths. These results were recently confirmed by the ACTT-2 trial. Due to paucity of studies and to the small size clinical series, the results of other immune therapies were not conclusive.
Conclusions: Beyond the supportive therapy, up to now the best therapeutic approach for COVID-19 may be a three-step combination therapy, including remdesivir 100 mg/day (200 mg loading dose on first day) in the first stage of the disease, and combined dexamethasone 6 mg/day plus baricitinib 4 mg/day to target the immune dysregulation triggered by the SARS-CoV-2 infection. The promising results of anakinra should be confirmed by the ongoing RCTs.
Conflict of interest statement
Authors have nothing to disclose.
Figures



References
-
- WHO. Coronavirus 2019. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re.... Accessed 14 Mar 2020.
-
- Ziegler CGK, Allon SJ, Nyquist SK, Mbano IM, Miao VN, Tzouanas CN, et al. SARS-CoV-2 receptor ACE2 is an interferon-stimulated gene in human airway epithelial cells and is detected in specific cell subsets across tissues. Cell. 2020;181(5):1016–1035.e19. doi: 10.1016/j.cell.2020.04.035. - DOI - PMC - PubMed
-
- Glowacka I, Bertram S, Müller MA, Allen P, Soilleux E, Pfefferle S, et al. Evidence that TMPRSS2 activates the severe acute respiratory syndrome coronavirus spike protein for membrane fusion and reduces viral control by the humoral immune response. J Virol. 2011;85(9):4122–4134. doi: 10.1128/jvi.02232-10. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
