

Stroke Care Trends During COVID-19 Pandemic in Zanjan Province, Iran. From the CASCADE Initiative: Statistical Analysis Plan and Preliminary Results
- PMID: 33069086
- PMCID: PMC7494258
- DOI: 10.1016/j.jstrokecerebrovasdis.2020.105321
Stroke Care Trends During COVID-19 Pandemic in Zanjan Province, Iran. From the CASCADE Initiative: Statistical Analysis Plan and Preliminary Results
Abstract
Background: The emergence of the COVID-19 pandemic has significantly impacted global healthcare systems and this may affect stroke care and outcomes. This study examines the changes in stroke epidemiology and care during the COVID-19 pandemic in Zanjan Province, Iran.
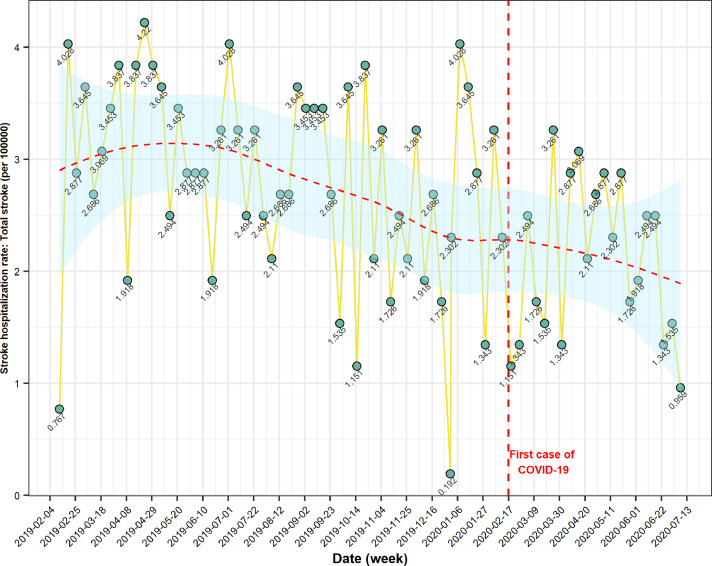
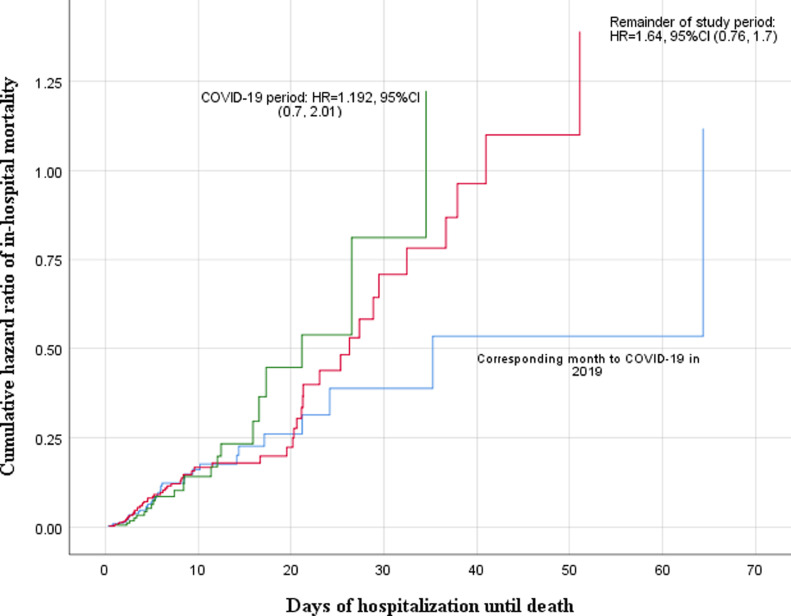
Methods: This study is part of the CASCADE international initiative. From February 18, 2019, to July 18, 2020, we followed ischemic and hemorrhagic stroke hospitalization rates and outcomes in Valiasr Hospital, Zanjan, Iran. We used a Bayesian hierarchical model and an interrupted time series analysis (ITS) to identify changes in stroke hospitalization rate, baseline stroke severity [measured by the National Institutes of Health Stroke Scale (NIHSS)], disability [measured by the modified Rankin Scale (mRS)], presentation time (last seen normal to hospital presentation), thrombolytic therapy rate, median door-to-needle time, length of hospital stay, and in-hospital mortality. We compared in-hospital mortality between study periods using Cox-regression model.
Results: During the study period, 1,026 stroke patients were hospitalized. Stroke hospitalization rates per 100,000 population decreased from 68.09 before the pandemic to 44.50 during the pandemic, with a significant decline in both Bayesian [Beta: -1.034; Standard Error (SE): 0.22, 95% CrI: -1.48, -0.59] and ITS analysis (estimate: -1.03, SE = 0.24, p < 0.0001). Furthermore, we observed lower admission rates for patients with mild (NIHSS < 5) ischemic stroke (p < 0.0001). Although, the presentation time and door-to-needle time did not change during the pandemic, a lower proportion of patients received thrombolysis (-10.1%; p = 0.004). We did not see significant changes in admission rate to the stroke unit and in-hospital mortality rate; however, disability at discharge increased (p < 0.0001).
Conclusion: In Zanjan, Iran, the COVID-19 pandemic has significantly impacted stroke outcomes and altered the delivery of stroke care. Observed lower admission rates for milder stroke may possibly be due to fear of exposure related to COVID-19. The decrease in patients treated with thrombolysis and the increased disability at discharge may indicate changes in the delivery of stroke care and increased pressure on existing stroke acute and subacute services. The results of this research will contribute to a similar analysis of the larger CASCADE dataset in order to confirm findings at a global scale and improve measures to ensure the best quality of care for stroke patients during the COVID-19 pandemic.
Keywords: COVID-19; Disability; Epidemiology; Mortality; Outcome; Stroke; Stroke care.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
References
-
- Adhanom Ghebreyesus T. We now have a name for the disease caused by the novel coronavirus: COVID-19 [Internet]. twitter . 2020 [cited 2020 Jul 22]. Available from: https://twitter.com/DrTedros/status/1227297754499764230.
-
- Martinez R, Lloyd-Sherlock P, Soliz P, Ebrahim S, Vega E, Ordunez P. Trends in premature avertable mortality from non-communicable diseases for 195 countries and territories, 1990-2017: a population-based study. Lancet Glob Health. 2020;8(4):e511–e523. - PubMed
