

CT and FDG-PET radiologic biomarkers in p16+ oropharyngeal squamous cell carcinoma patients treated with definitive chemoradiotherapy
- PMID: 33069764
- PMCID: PMC10326862
- DOI: 10.1016/j.radonc.2020.10.006
CT and FDG-PET radiologic biomarkers in p16+ oropharyngeal squamous cell carcinoma patients treated with definitive chemoradiotherapy
Abstract
Purpose: To assess associations between imaging biomarkers from standard of care pre-treatment CT and FDG-PET scans and locoregional (LR) and distant metastatic (DM) recurrences in patients with p16+ oropharyngeal squamous cell carcinoma (OPSCC) treated with definitive chemoradiotherapy (CRT).
Methods: An institutional database from a single NCI-designated cancer center identified 266 patients with p16+ OPSCC treated with definitive CRT in our department from 2005 to 2016 with evaluable pre-treatment FDG-PET scans. Quantitative SUV metrics and qualitative imaging metrics were determined from FDG-PET and CT scans, while clinical characteristics were abstracted from the medical record. Associations between clinical/imaging features and time to LR (TTLRF) or DM (TTDMF) failure and overall survival (OS) were assessed using univariable Cox regression and penalized stepwise regression for multivariable analyses (MVA).
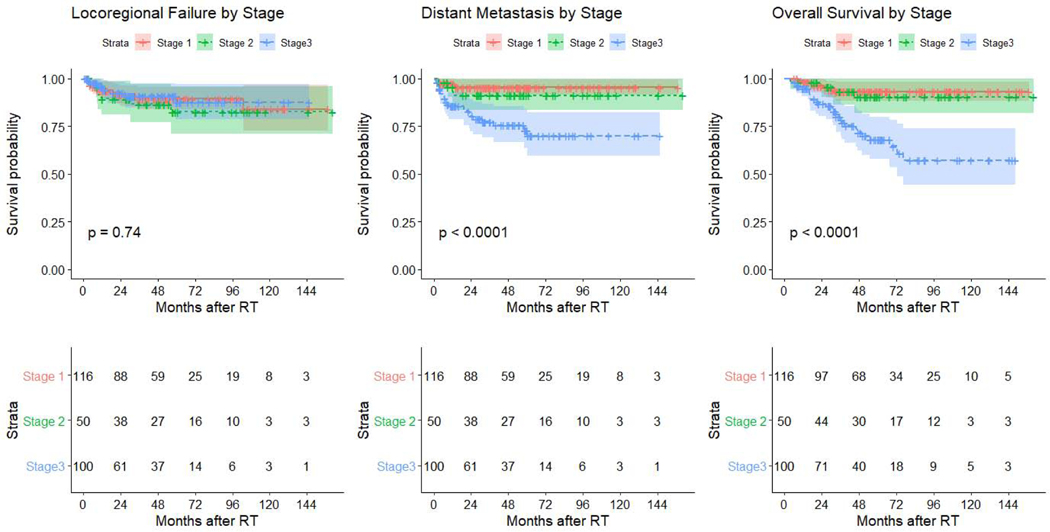
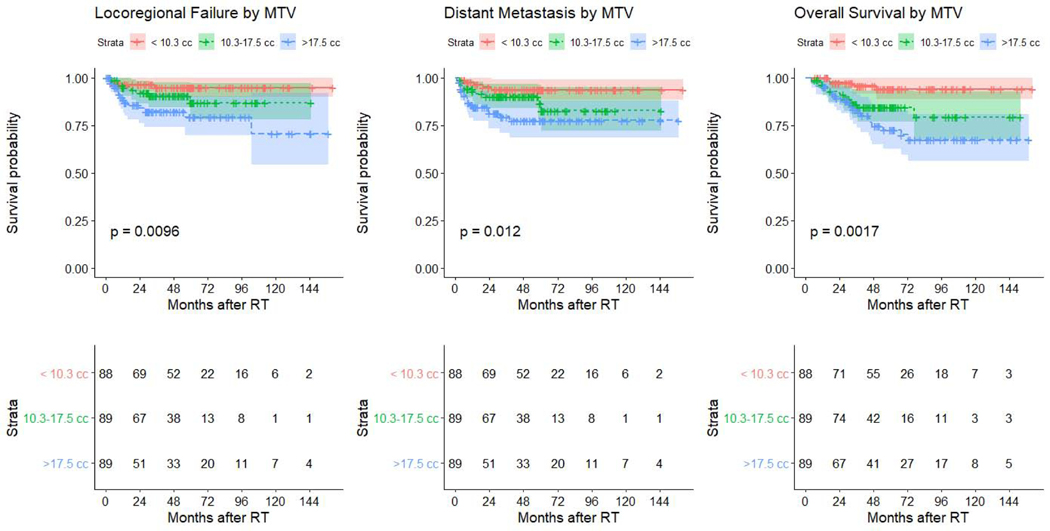
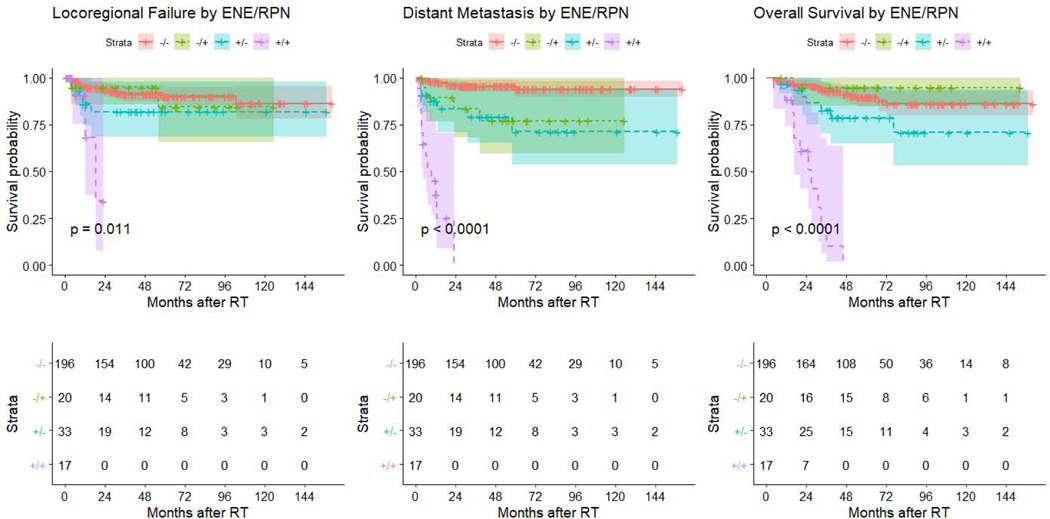
Results: There were 27 LR and 32 DM recurrences as incident failures. Imaging biomarkers were significantly associated with TTLRF, TTDMF and OS. FDG-PET metrics outperformed CT and clinical metrics for TTLRF, with metabolic tumor volume being the only significant feature selected on MVA: C-index = 0.68 (p = 0.01). Radiographic extranodal extension (rENE), positive retropharyngeal nodes (RPN+), and clinical stage were significant on MVA for TTDMF: C-index = 0.84 (p < 0.001). rENE, group stage, and RPN+ were significant on MVA for OS: C-index = 0.77 (p < 0.001).
Conclusions: In the largest study to date of uniformly treated patients with CRT to evaluate both pretreatment CT and FDG-PET, radiographic biomarkers were significantly associated with TTLRF, TTDMF and OS among patients with p16+ OPSCC treated with CRT. CT metrics performed best to predict TTDMF, while FDG-PET metrics showed improved prediction for LRRFS. These metrics may help identify candidates for treatment intensification or de-escalation of therapy.
Statement of translational relevance: Pre-treatment imaging features from standard-of-care PET/CT imaging show promise for predicting long-term outcomes following HPV-associated oropharynx cancer (HPV-OPC) therapy. This study comprehensively characterizes qualitative and quantitative pre-treatment imaging metrics associated with time to pattern-specific failure in a cohort of 266 patients treated uniformly with definitive chemoradiation. Multivariate analysis (MVA) for time to locoregional failure (TTLRF), time to distant metastatic failure (TTDMF), and overall survival (OS) was performed. FDG-PET metrics outperformed CT and clinical metrics for TTLRF. CT radiographic extranodal extension, positive retropharyngeal nodes, and stage strongly predicted TTDMF (combined C-index = 0.84, log rank p < 0.001). Number of smoking pack-years complemented clinical and imaging features only in patients without radiographic extranodal extension or positive retropharyngeal nodes. Time to pattern-specific failure is important for guiding treatment de-escalation strategies, which intend to reduce treatment-related toxicity in patients with relatively long expected survival times. This study suggests that PET/CT features should play a crucial role in future de-escalation trials and management of HPV-OPC patients.
Keywords: Computed tomography; FDG-PET; HPV cancers; Imaging biomarkers; Oropharynx.
Copyright © 2020 Elsevier B.V. All rights reserved.
Figures
References
-
- Fakhry C, Zhang Q, Gillison ML, Nguyen-Tan PF, Rosenthal DI, Weber RS, et al. (2019). “Validation of NRG oncology/RTOG-0129 risk groups for HPV-positive and HPV-negative oropharyngeal squamous cell cancer: Implications for risk-based therapeutic intensity trials.” Cancer 125(12): 2027–38. - PMC - PubMed
-
- Rosenthal DI, Harari PM, Giralt J, Bell D, Raben D, Liu J, et al. (2016). “Association of Human Papillomavirus and p16 Status With Outcomes in the IMCL-9815 Phase III Registration Trial for Patients With Locoregionally Advanced Oropharyngeal Squamous Cell Carcinoma of the Head and Neck Treated With Radiotherapy With or Without Cetuximab.” J Clin Oncol 34(12): 1300–8. - PMC - PubMed
-
- O’Sullivan B, Huang SH, Su J, Garden AS, Sturgis EM, Dahlstrom K, et al. (2016). “Development and validation of a staging system for HPV-related oropharyngeal cancer by the International Collaboration on Oropharyngeal cancer Network for Staging (ICON-S): a multicentre cohort study.” The Lancet Oncology 17(4): 440–51. - PubMed
-
- Lydiatt WM, Patel SG, O’Sullivan B, Brandwein MS, Ridge JA, Migliacci JC, et al. (2017). “Head and neck cancers—major changes in the American Joint Committee on cancer eighth edition cancer staging manual.” CA: A Cancer Journal for Clinicians 67(2): 122–37. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
