

The role of dysregulated immune responses in COVID-19 pathogenesis
- PMID: 33069815
- PMCID: PMC7561578
- DOI: 10.1016/j.virusres.2020.198197
The role of dysregulated immune responses in COVID-19 pathogenesis
Abstract
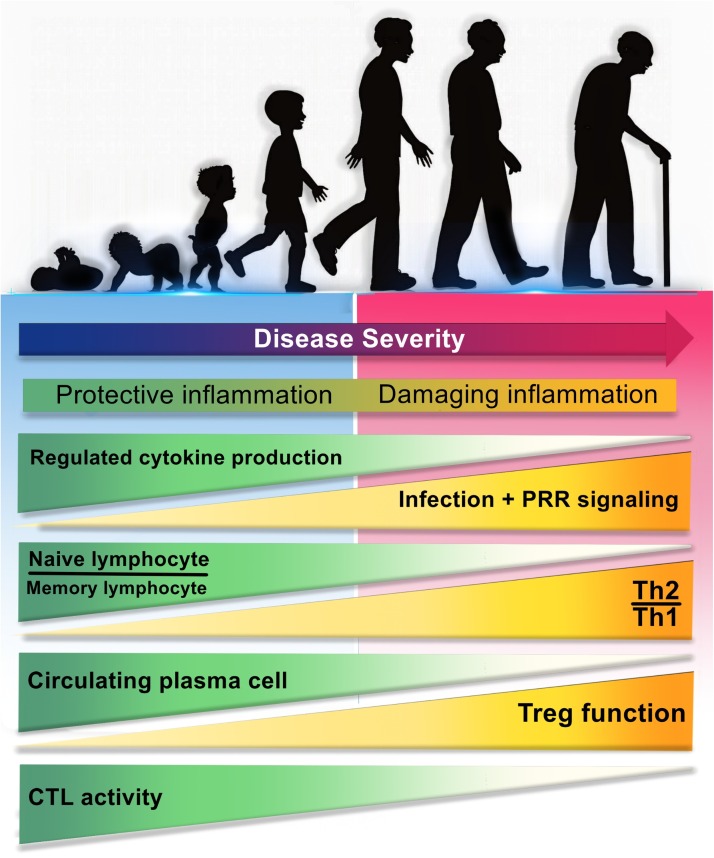
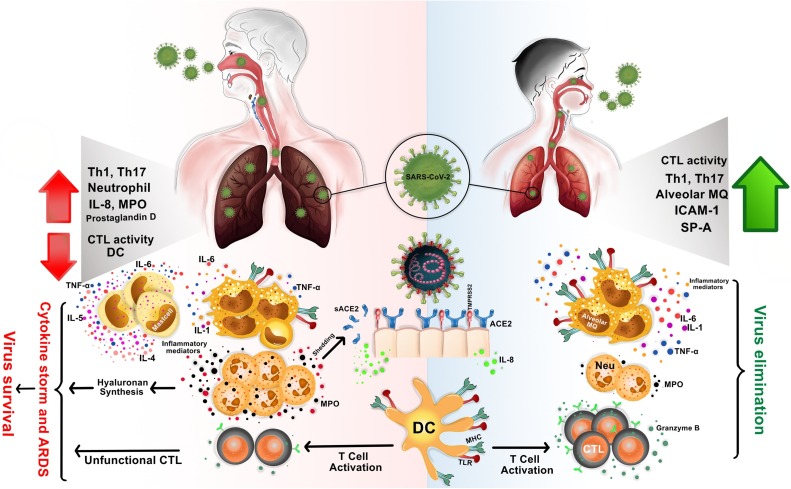
The coronavirus disease-2019 (COVID-19) which caused by severe acute respiratory syndrome-related coronavirus (SARS-CoV-2), is a pandemic threat to global public health. It has a wide spectrum of clinical manifestations from mild to critical illness, the most serious of which is the complications of acute respiratory distress syndrome (ARDS). SARS-CoV-2 infection appears mild in infants and children, however, in adults, it can lead to serious consequences. In this review, we highlighted the differences between the immune responses of the lung in children and adults, immune dysregulation and their possible role in clinical manifestations in COVID-19. There is a reduction in population of immunocompetent cells during aging and subsequently induced ineffective inflammation in the faces of some infections. Dysregulation in the immune system can lead to an unappropriated local and systemic immune responses and subsequently the rapid spread of the virus, leading to severe COVID-19 disease. Therefore, recognizing the differences in the immune responses of various hosts as well as to improve the immune system disorder should always be part of research and treatment protocols.
Keywords: COVID-19; Immune dysregulation; Immunopathogenesis; SARS-CoV-2.
Copyright © 2020. Published by Elsevier B.V.
Conflict of interest statement
The authors declare no conflicts of interests
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
