

Modelling the impact of the mandatory use of face coverings on public transport and in retail outlets in the UK on COVID-19-related infections, hospital admissions and mortality
- PMID: 33070412
- PMCID: PMC7645947
- DOI: 10.1111/ijcp.13768
Modelling the impact of the mandatory use of face coverings on public transport and in retail outlets in the UK on COVID-19-related infections, hospital admissions and mortality
Abstract
Introduction: The rapid spread of the pandemic caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2/)(COVID-19) virus resulted in governments around the world instigating a range of measures, including mandating the wearing of face coverings on public transport/in retail outlets.
Methods: We developed a sequential assessment of the risk reduction provided by face coverings using a step-by-step approach. The UK Office of National Statistics (ONS) Population Survey data were utilised to determine the baseline total number of community-derived infections. These were linked to reported hospital admissions/hospital deaths to create case admission risk ratio and admission-related fatality rate. We evaluated published evidence to establish an infection risk reduction for face coverings. We calculated an Infection Risk Score (IRS) for a number of common activities and related it to the effectiveness of reducing infection and its consequences, with a face covering, and evaluated their effect when applied to different infection rates over 3 months from July 24, 2020, when face coverings were made compulsory in England on public transport/retail outlets.
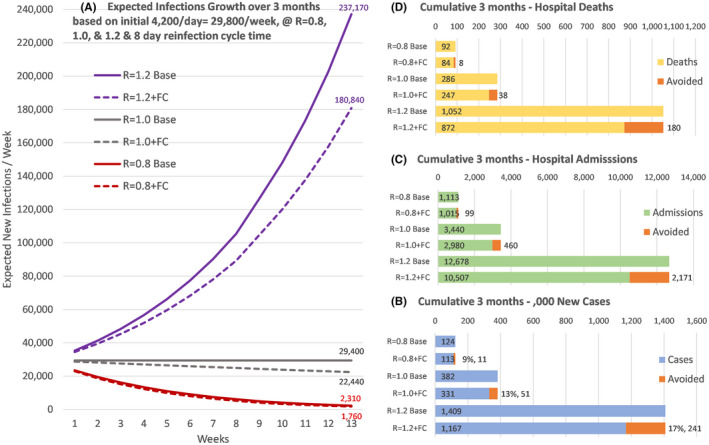
Results: We show that only 7.3% of all community-based infection risk is associated with public transport/retail outlets. In the week of July 24, The reported weekly community infection rate was 29 400 new cases at the start (July 24). The rate of growth in hospital admissions and deaths for England was around -15%/week, suggesting the infection rate, R, in the most vulnerable populations was just above 0.8. In this situation, average infections over the evaluated 13 week follow-up period, would be 9517/week with face covering of 40% effectiveness, thus, reducing average infections by 844/week, hospital admissions by 8/week and deaths by 0.6/week; a fall of 9% over the period total. If, however, the R-value rises to 1.0, then, average community infections would stay at 29 400/week and mandatory face coverings could reduce average weekly infections by 3930, hospital admissions by 36 and deaths by 2.9/week; a 13% reduction. If the R-value rose and stayed at 1.2, then, expected average community-derived hospital admissions would be 975/week and 40% effective face coverings would reduce this by 167/week and reduce possible expected hospital deaths from 80/week to 66/week. These reductions should be seen in the context that there was an average of 102 000/week all-cause hospital emergency admissions in England in June and 8900 total reported deaths in the week ending August 7, 2020.
Conclusion: We have illustrated that the policy on mandatory use of face coverings in retail outlets/on public transport may have been very well followed, but may be of limited value in reducing hospital admissions and deaths, at least at the time that it was introduced, unless infections begin to rise faster than currently seen. The impact appears small compared with all other sources of risk, thereby raising questions regarding the effectiveness of the policy.
© 2020 The Authors. International Journal of Clinical Practice published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Theory-based Trial to Promote Uptake and Sustained Use of Face Coverings During the COVID-19 Pandemic.Ann Behav Med. 2023 Oct 16;57(11):921-928. doi: 10.1093/abm/kaad039. Ann Behav Med. 2023. PMID: 37656890 Free PMC article. Clinical Trial.
-
Association of tiered restrictions and a second lockdown with COVID-19 deaths and hospital admissions in England: a modelling study.Lancet Infect Dis. 2021 Apr;21(4):482-492. doi: 10.1016/S1473-3099(20)30984-1. Epub 2020 Dec 24. Lancet Infect Dis. 2021. PMID: 33357518 Free PMC article.
-
Voluntary risk mitigation behaviour can reduce impact of SARS-CoV-2: a real-time modelling study of the January 2022 Omicron wave in England.BMC Med. 2023 Jan 19;21(1):25. doi: 10.1186/s12916-022-02714-5. BMC Med. 2023. PMID: 36658548 Free PMC article.
-
The Great Mask Debate: A Debate That Shouldn't Be a Debate at All.WMJ. 2020 Dec;119(4):229-239. WMJ. 2020. PMID: 33428832 Review.
-
Can Copper Products and Surfaces Reduce the Spread of Infectious Microorganisms and Hospital-Acquired Infections?Materials (Basel). 2021 Jun 22;14(13):3444. doi: 10.3390/ma14133444. Materials (Basel). 2021. PMID: 34206230 Free PMC article. Review.
Cited by
-
The emission and dynamics of droplets from human expiratory activities and COVID-19 transmission in public transport system: A review.Build Environ. 2022 Jul 1;219:109224. doi: 10.1016/j.buildenv.2022.109224. Epub 2022 May 24. Build Environ. 2022. PMID: 35645454 Free PMC article. Review.
-
Effects of transport-related COVID-19 policy measures: A case study of six developed countries.Transp Policy (Oxf). 2021 Sep;110:37-57. doi: 10.1016/j.tranpol.2021.05.013. Epub 2021 May 30. Transp Policy (Oxf). 2021. PMID: 34608358 Free PMC article.
-
Changes in prescribing of psychotropic vs some physical health medication in primary care through the COVID-19 pandemic in England: a national-level survey.J Pharm Policy Pract. 2023 Dec 21;16(1):169. doi: 10.1186/s40545-023-00655-9. J Pharm Policy Pract. 2023. PMID: 38124123 Free PMC article.
-
Patterns of Virus Exposure and Presumed Household Transmission among Persons with Coronavirus Disease, United States, January-April 2020.Emerg Infect Dis. 2021 Sep;27(9):2323-2332. doi: 10.3201/eid2709.204577. Epub 2021 Jun 30. Emerg Infect Dis. 2021. PMID: 34193337 Free PMC article.
-
Changes in primary care visits for respiratory illness during the COVID-19 pandemic: a multinational study by the International Consortium of Primary Care Big Data Researchers (INTRePID).Front Med (Lausanne). 2024 Jun 17;11:1343646. doi: 10.3389/fmed.2024.1343646. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38952865 Free PMC article.
References
-
- World Health Organisation . Advice on the use of masks in the context of COVID‐19: interim guidance; June 5, 2020. https://apps.who.int/iris/handle/10665/332293. Accessed October 6, 2020.
-
- DELVE: Report on face masks for the general public; April 2020. https://www.gov.uk/government/publications/delve‐report‐on‐face‐masks‐fo.... Accessed October 6, 2020.
-
- UK Department of Health and Social Care . Face coverings: when to wear one and how to make your own; July, 2020. https://www.gov.uk/government/publications/face‐coverings‐when‐to‐wear‐o.... Accessed August 31, 2020.
-
- Royal Society . Face masks and coverings for the general public: behavioural knowledge, effectiveness of cloth coverings and public messaging. 2020. https://royalsociety.org/‐/media/policy/projects/set‐c/set‐c‐facemasks.p...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous