

Recommendations for use of antigenic tests in the diagnosis of acute SARS-CoV-2 infection in the second pandemic wave: attitude in different clinical settings
- PMID: 33070578
- PMCID: PMC7712344
- DOI: 10.37201/req/120.2020
Recommendations for use of antigenic tests in the diagnosis of acute SARS-CoV-2 infection in the second pandemic wave: attitude in different clinical settings
Abstract
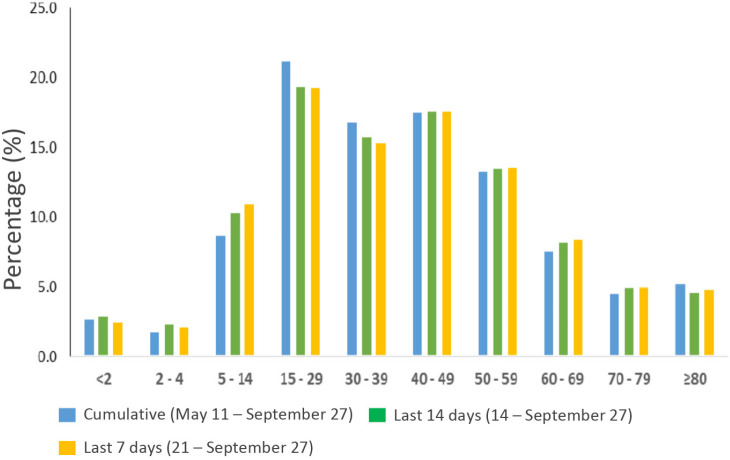
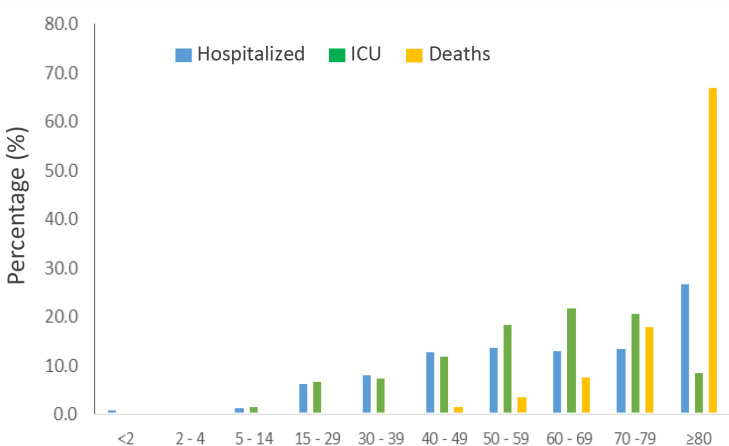
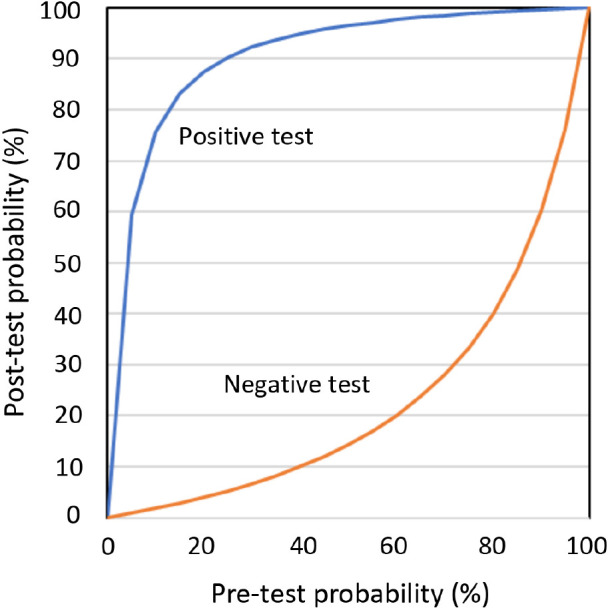
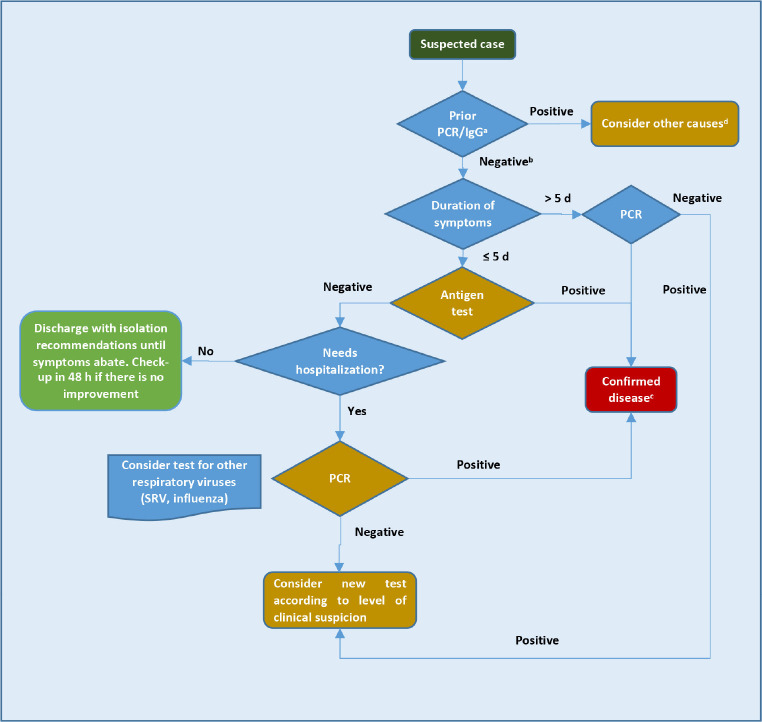
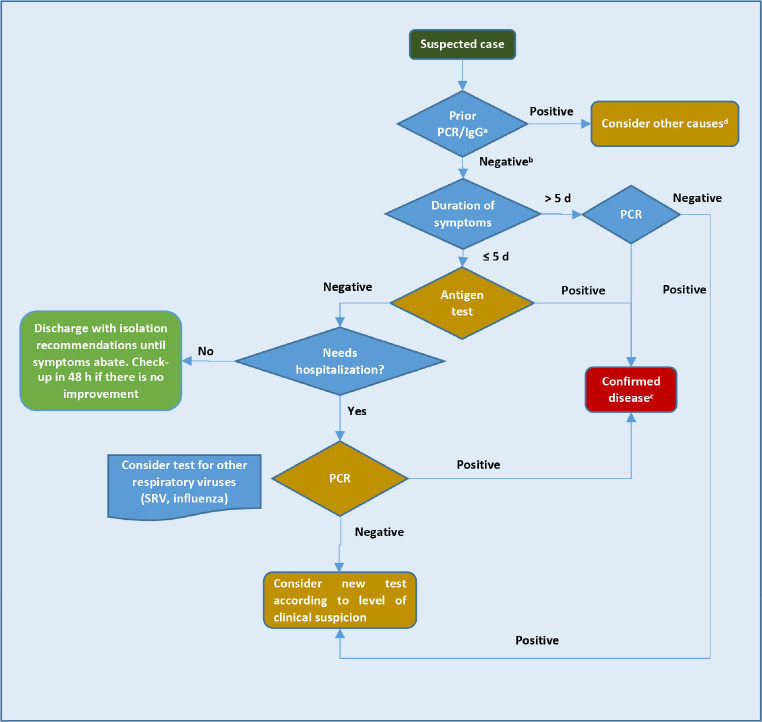
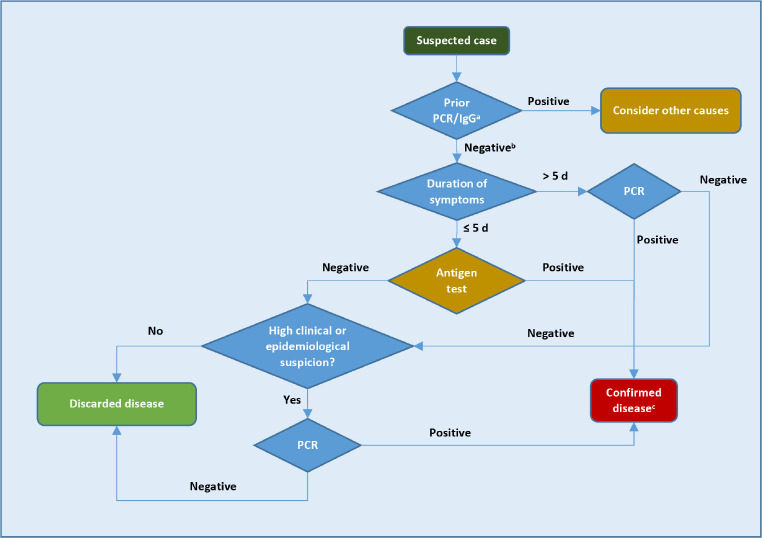
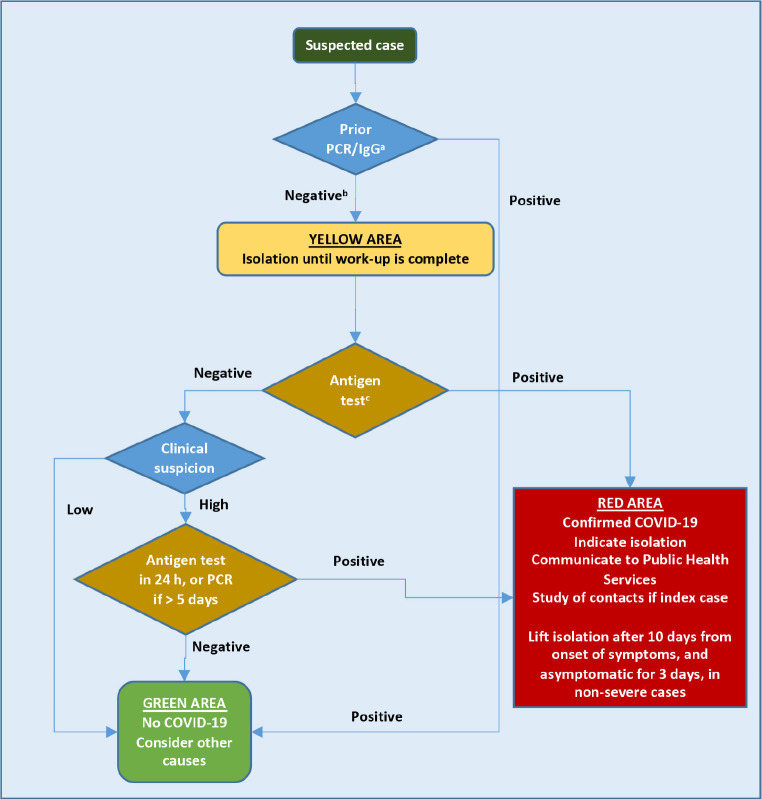
The high transmissibility of SARS-CoV-2 before and shortly after the onset of symptoms suggests that only diagnosing and isolating symptomatic patients may not be sufficient to interrupt the spread of infection; therefore, public health measures such as personal distancing are also necessary. Additionally, it will be important to detect the newly infected individuals who remain asymptomatic, which may account for 50% or more of the cases. Molecular techniques are the "gold standard" for the diagnosis of SARS-CoV-2 infection. However, the massive use of these techniques has generated some problems. On the one hand, the scarcity of resources (analyzers, fungibles and reagents), and on the other the delay in the notification of results. These two facts translate into a lag in the application of isolation measures among cases and contacts, which favors the spread of the infection. Antigen detection tests are also direct diagnostic methods, with the advantage of obtaining the result in a few minutes and at the very "pointof-care". Furthermore, the simplicity and low cost of these tests allow them to be repeated on successive days in certain clinical settings. The sensitivity of antigen tests is generally lower than that of nucleic acid tests, although their specificity is comparable. Antigenic tests have been shown to be more valid in the days around the onset of symptoms, when the viral load in the nasopharynx is higher. Having a rapid and real-time viral detection assay such as the antigen test has been shown to be more useful to control the spread of the infection than more sensitive tests, but with greater cost and response time, such as in case of molecular tests. The main health institutions such as the WHO, the CDC and the Ministry of Health of the Government of Spain propose the use of antigenic tests in a wide variety of strategies to respond to the pandemic. This document aims to support physicians involved in the care of patients with suspected SC2 infection, in the context of a growing incidence in Spain since September 2020, which already represents the second pandemic wave of COVID-19.
Keywords: COVID-19; PCR; SARS-CoV2; antigenic test; diagnosis; emergency departments; microbiology; nursing home and long-term facilities; pediatrics; primary care.
©The Author 2020. Published by Sociedad Española de Quimioterapia. This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)(https://creativecommons.org/licenses/by-nc/4.0/).
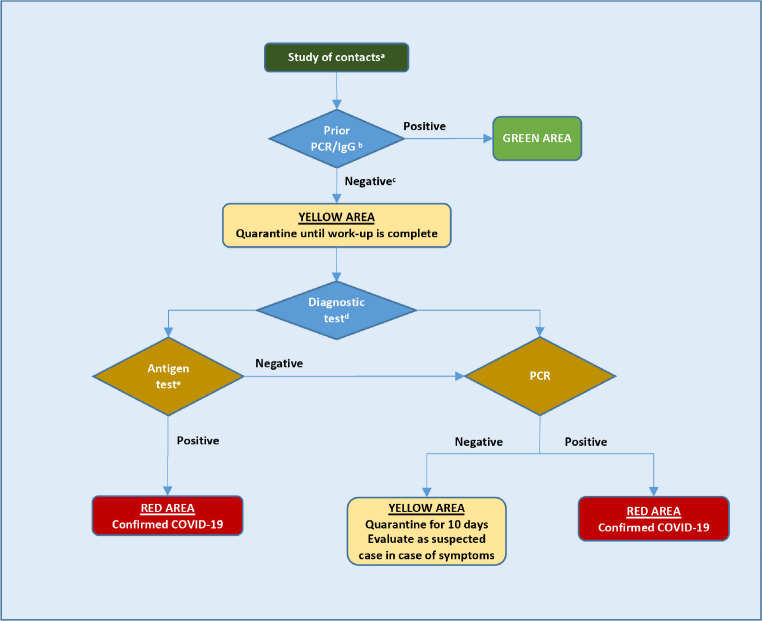
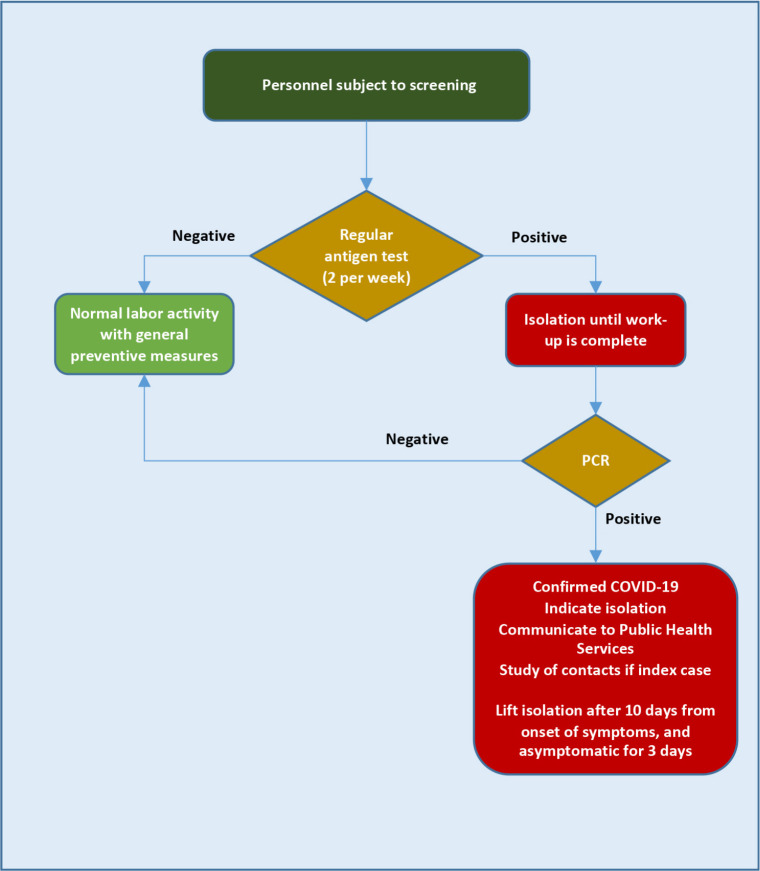
Figures
References
-
- Instituto de Salud Carlos III. Estrategia de detección precoz, vigilancia y control de COVID-19. 25 de septiembre de 2020. Disponible en (consultado el 1 de octubre de 2020): https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual...
-
- Instituto de Salud Carlos III. Informe nº 30. Situación de COVID-19 en España. 11 de mayo de 2020. Disponible en (consultado el 29/09/2020): https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/...
-
- Instituto de Salud Carlos III. Informe nº 47. Situación de COVID-19 en España. Casos diagnosticados a partir 10 de mayo. 7 de octubre de 2020. Disponible en (consultado el 10/10/2020): https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/...
-
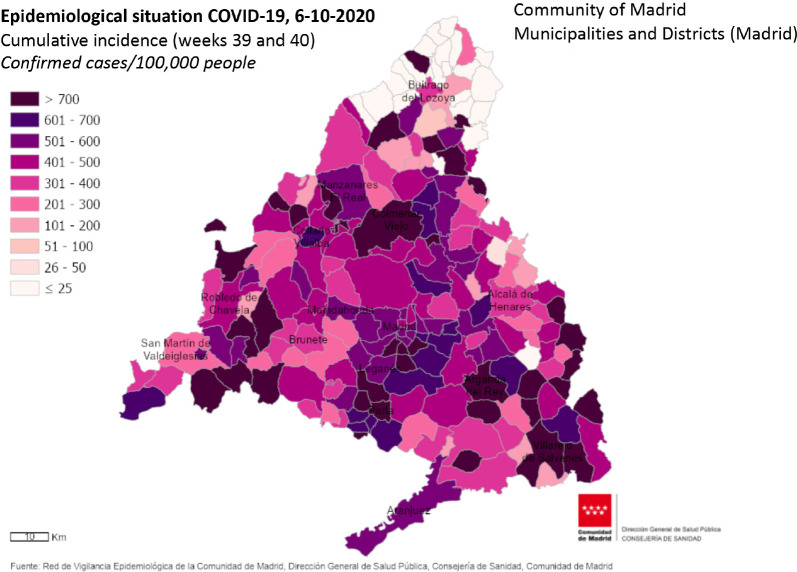
- Red de Vigilancia Epidemiológica de la CM. Semana 39. Infección por el nuevo coronavirus COVID-19 (Datos provisionales). 29 de septiembre de 2020: Disponible en (consultado el 29/09/2020): https://www.comunidad.madrid/sites/default/files/doc/sanidad/epid/inform...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
