

Cerebral venous thrombosis in COVID-19-associated coagulopathy: A case report
- PMID: 33070913
- PMCID: PMC7377797
- DOI: 10.1016/j.jocn.2020.07.038
Cerebral venous thrombosis in COVID-19-associated coagulopathy: A case report
Abstract
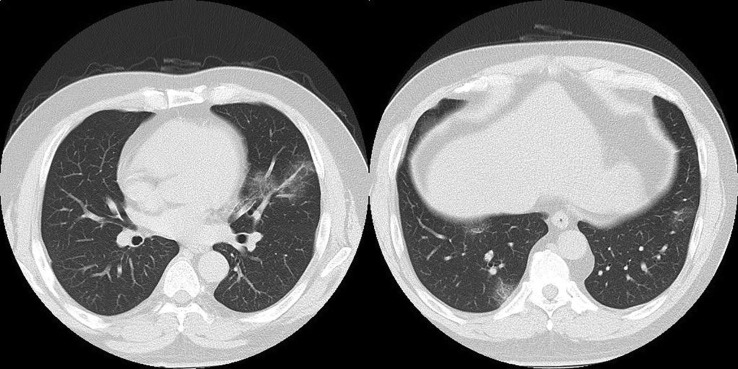
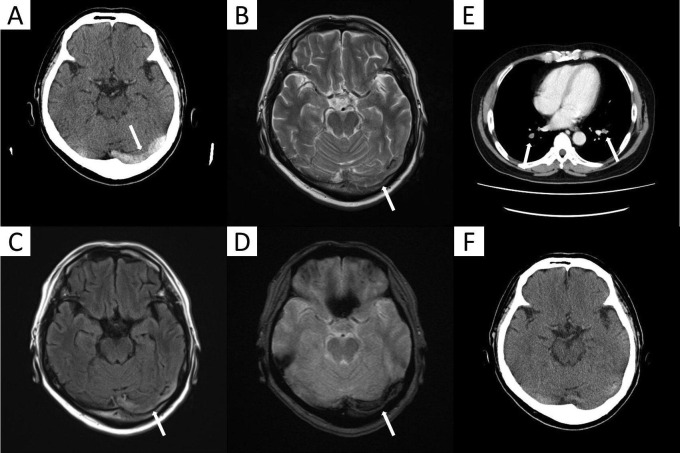
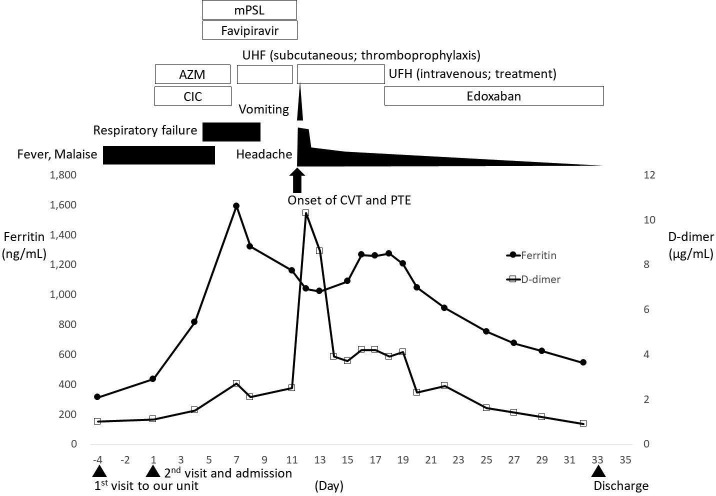
COVID-19 is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first reported in Wuhan, China in December 2019, and is ongoing pandemic. While a majority of patients with SARS-CoV-2 infection shows asymptomatic or mild disease, hospitalized patients can develop critical condition, such as pneumonia, sepsis, and respiratory failure. Some cases deteriorate into sever systemic disease and multiorgan failure. Many patients of severe COVID-19 show hypercoagulable state and complicate with venous thromboembolism and atrial thrombosis. We herein reported a case of COVID-19 who developed cerebral venous thrombosis (CVT) co-incidence with pulmonary thromboembolism (PTE). A 56-year-old Japanese man was presented with fever and malaise and diagnosed with COVID-19. He was treated with ciclesonide and azithromycin, but his respiratory condition deteriorated. Thus, systemic corticosteroids and favipiravir were initiated and these treatments resulted in afebrile state, improving malaise and respiratory failure. However, he suddenly developed severe headache and vomiting with increased concentration of D-dimer. Brain CT and MRI showed typical images of CVT in the left transvers sinus and CT pulmonary angiography showed PE. Administration of unfractionated heparin followed by edoxaban treatment reduced the levels of D-dimer and improved his clinical presentation and thrombosis. Monitoring coagulopathy is important in COVID-19 patients and in case of venous thromboembolism, including cerebral venous system, appropriate anticoagulant therapy should be initiated.
Keywords: COVID-19; Cerebral venous thrombosis; D-dimer; Edoxaban; Pulmonary thromboembolism.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Panigada M., Bottino N., Tagliabue P., Grasselli G., Novembrino C., Chantarangkul V., Pesenti A., Peyvandi F., Tripodi A. Hypercoagulability of COVID‐19 patients in intensive care unit: a report of thromboelastography findings and other parameters of hemostasis. J Thromb Haemost. 2020;18(7):1738–1742. doi: 10.1111/jth.v18.710.1111/jth.14850. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
