

Effect of surgical versus medical therapy on estimated cardiovascular event risk among adolescents with type 2 diabetes and severe obesity
- PMID: 33071178
- PMCID: PMC8007282
- DOI: 10.1016/j.soard.2020.09.002
Effect of surgical versus medical therapy on estimated cardiovascular event risk among adolescents with type 2 diabetes and severe obesity
Abstract
Background: Cardiovascular disease (CVD) remains the leading cause of mortality in type 2 diabetes (T2D). Better interventions are needed to mitigate the high lifetime risk for CVD in youth T2D.
Objective: To compare 30-year risk for CVD events in 2 cohorts of adolescents with T2D and severe obesity undergoing medical or surgical treatment of T2D.
Setting: Longitudinal multicenter studies at University hospitals.
Methods: A secondary analysis of data collected from the participants with T2D enrolled in the Teen-Longitudinal Assessment of Bariatric Surgery (Teen-LABS, n = 30) and participants of similar age and racial distribution from the Treatment Options of Type 2 Diabetes in Adolescents and Youth (TODAY, n = 63) studies was performed. Teen-LABS participants underwent metabolic bariatric surgery (MBS). TODAY participants were randomized to metformin alone or in combination with rosiglitazone or intensive lifestyle intervention, with insulin therapy given for glycemic progression. A 30-year CVD event score developed by the Framingham Heart Study was the primary outcome, assessed at baseline (preoperatively for Teen-LABS), 1 year, and 5 years of follow-up.
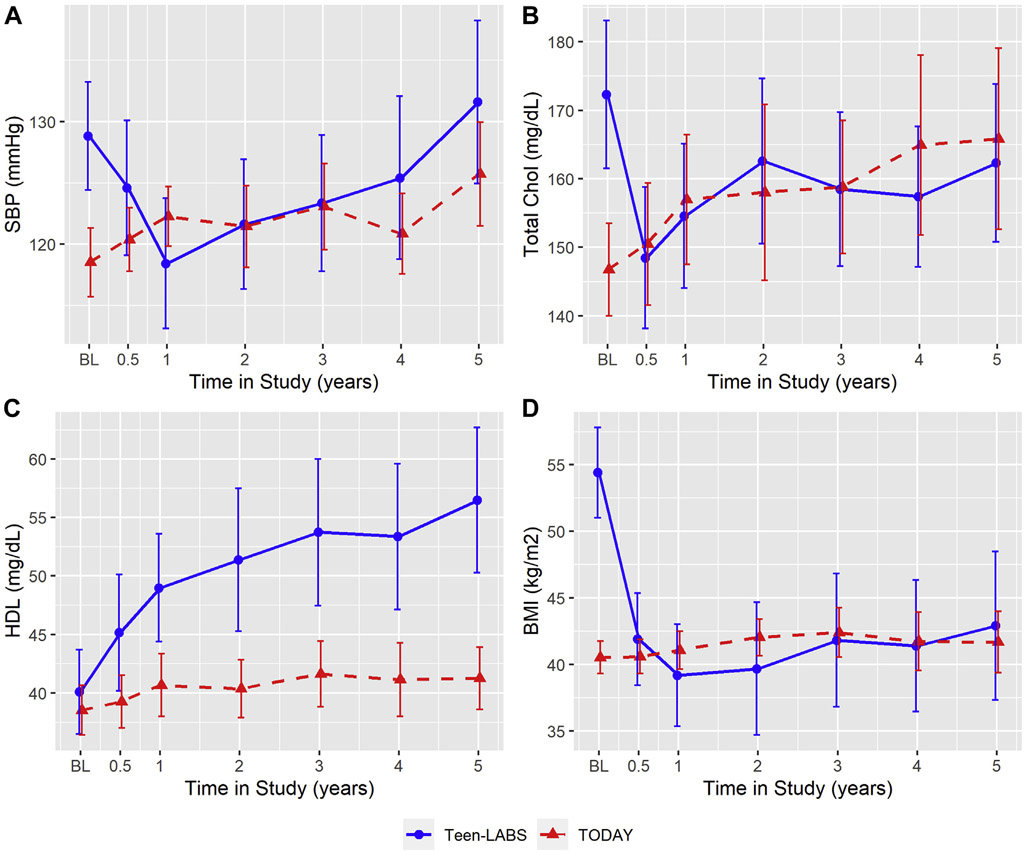
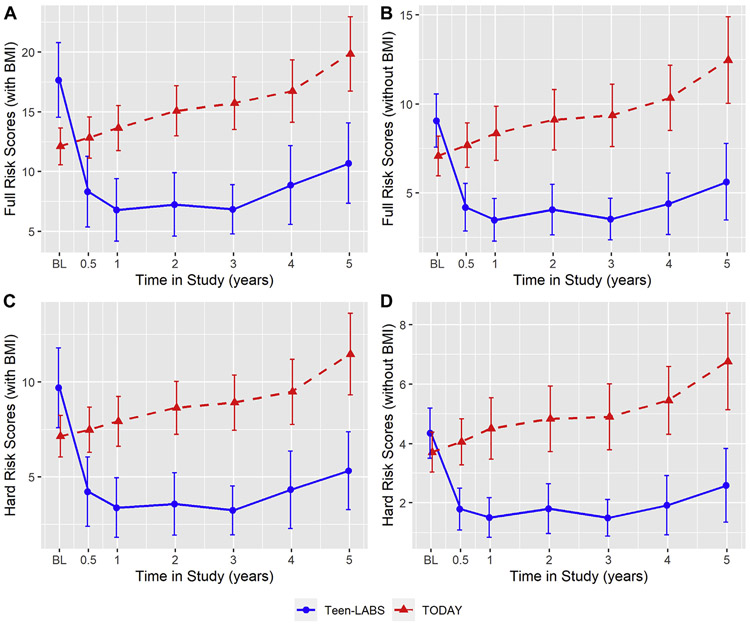
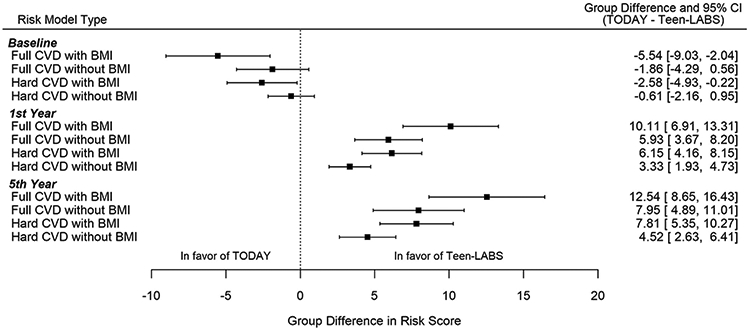
Results: Participants with T2D from Teen-LABS (n = 30; mean ± SD age = 16.9 ± 1.3 yr; 70% female; 60% white; body mass index (BMI) = 54.4 ± 9.5 kg/m2) and TODAY (n = 63; 15.3 ± 1.3 yr; 56% female; 71% white; BMI 40.5 ± 4.9 kg/m2) were compared. The likelihood of CVD events was higher in Teen-LABS versus TODAY at baseline (17.66 [1.59] versus 12.11 [.79]%, adjusted P = .002). One year after MBS, event risk was significantly lower in Teen-LABS versus TODAY (6.79 [1.33] versus 13.64 [0.96]%, adjusted P < .0001), and sustained at 5 years follow-up (adjusted P < .0001).
Conclusion: Despite higher pretreatment risk for CVD events, treatment with MBS resulted in a reduction in estimated CVD event risks, whereas medical therapy associated with an increase in risk among adolescents with T2D and severe obesity.
Keywords: Cardiovascular disease; Medical therapy; Metabolic bariatric surgery; Prediction; Severe obesity; Type 2 diabetes.
Copyright © 2020 American Society for Bariatric Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Why are adolescents with obesity and diabetes not having bariatric surgery earlier?Surg Obes Relat Dis. 2021 Jan;17(1):33-35. doi: 10.1016/j.soard.2020.10.005. Epub 2020 Oct 15. Surg Obes Relat Dis. 2021. PMID: 33218902 No abstract available.
References
-
- Tancredi M, Rosengren A, Svensson A-M, et al. Excess mortality among persons with type 2 diabetes. N Engl J Med 2015;373(18): 1720–32. - PubMed
-
- Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998;339(4):229–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 RR025780/RR/NCRR NIH HHS/United States
- M01 RR000036/RR/NCRR NIH HHS/United States
- U01 DK061242/DK/NIDDK NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- U01 DK061212/DK/NIDDK NIH HHS/United States
- M01 RR014467/RR/NCRR NIH HHS/United States
- U01 DK061230/DK/NIDDK NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- M01 RR000084/RR/NCRR NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- U01 DK061254/DK/NIDDK NIH HHS/United States
- UL1 RR024139/RR/NCRR NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- P30 DK048520/DK/NIDDK NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- UL1 RR024153/RR/NCRR NIH HHS/United States
- UM1 DK072493/DK/NIDDK NIH HHS/United States
- M01 RR000069/RR/NCRR NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- K23 DK116720/DK/NIDDK NIH HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- K24 HL145076/HL/NHLBI NIH HHS/United States
- M01 RR000125/RR/NCRR NIH HHS/United States
- U01 DK061239/DK/NIDDK NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
