

A Cecal Mucormycosis Mass Mimicking Colon Cancer in a Patient with Renal Transplant: A Case Report and Literature Review
- PMID: 33071279
- PMCID: PMC7585455
- DOI: 10.12659/AJCR.926325
A Cecal Mucormycosis Mass Mimicking Colon Cancer in a Patient with Renal Transplant: A Case Report and Literature Review
Abstract
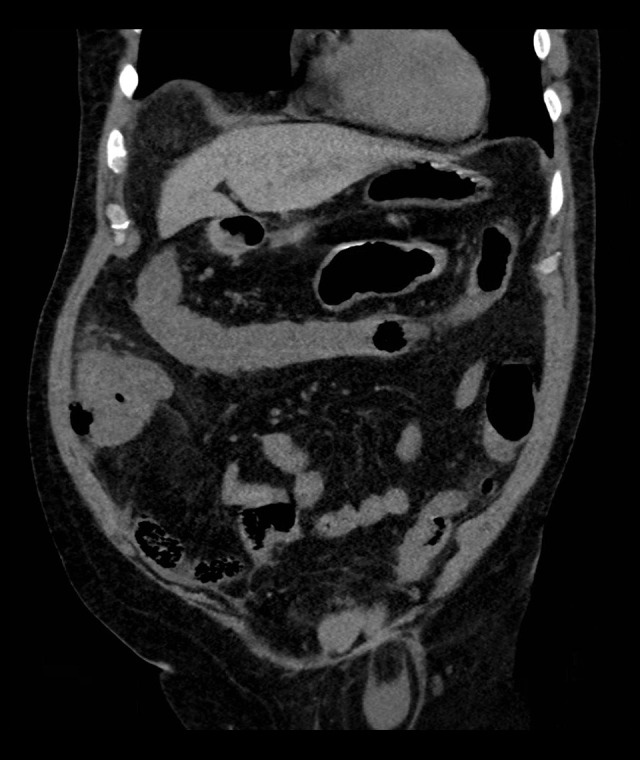
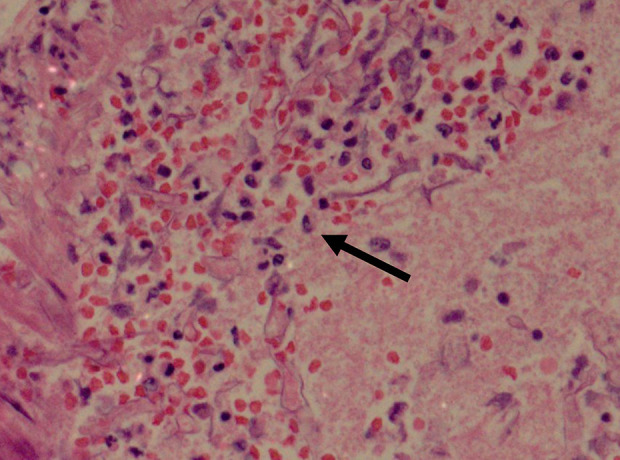
BACKGROUND Mucormycosis is a rare, invasive, and opportunistic fungal infection that occurs in the setting of neutropenia, immune deficiency, solid-organ transplant, and iron overload. The gastrointestinal system is a rare site of mucormycosis, and gastrointestinal mucormycosis is associated with high mortality and accounts for 4-7% of all cases. CASE REPORT We present the case of a 64-year-old hypertensive man with transfusion-dependent myelodysplastic syndrome who underwent renal transplant surgery 11 years ago. He also was taking maintenance Deferasirox for iron overload. He presented with a 2-day history of right lower-quadrant abdominal pain, nausea, vomiting, and non-bloody diarrhea. An abdominal examination revealed guarding and a 5×6 cm mass in the right iliac fossa. A CT scan of the abdomen showed signs of perforation of a cecal mass. As the patient was unstable, emergency right hemicolectomy and end ileostomy were performed. After the surgery, the patient was moved to the Intensive Care Unit (ICU) and a broad-spectrum antibiotic was administered. Histopathological examination results received on postoperative day 5 showed broad pauciseptate hyphae with substantial blood-vessel infiltration, suggestive of mucormycosis. Amphotericin B was started; however, on the same day, his condition deteriorated and he was moved back to the ICU. Despite maximum cardiorespiratory support, he had multiorgan failure and died. CONCLUSIONS Gastrointestinal mucormycosis presentation is non-specific, the diagnosis is often made late or is missed, and mortality remains high. High clinical suspicion, early diagnosis, and combined antifungal and surgical treatment is the best way to reduce mortality and improve survival.
Conflict of interest statement
Figures


References
-
- Almyroudis NG, Sutton DA, Linden P, et al. Zygomycosis in solid organ transplant recipients in a tertiary transplant center and review of the literature. Am J Transplant. 2006;6:2365–74. - PubMed
-
- Frater JL, Hall GS, Procop GW. Histologic features of zygomycosis: Emphasis on perineural invasion and fungal morphology. Arch Pathol Lab Med. 2001;125:375–78. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
