

Single-Center Experience With the Bare p48MW Low-Profile Flow Diverter and Its Hydrophilically Covered Version for Treatment of Bifurcation Aneurysms in Distal Segments of the Anterior and Posterior Circulation
- PMID: 33071937
- PMCID: PMC7538783
- DOI: 10.3389/fneur.2020.01050
Single-Center Experience With the Bare p48MW Low-Profile Flow Diverter and Its Hydrophilically Covered Version for Treatment of Bifurcation Aneurysms in Distal Segments of the Anterior and Posterior Circulation
Abstract
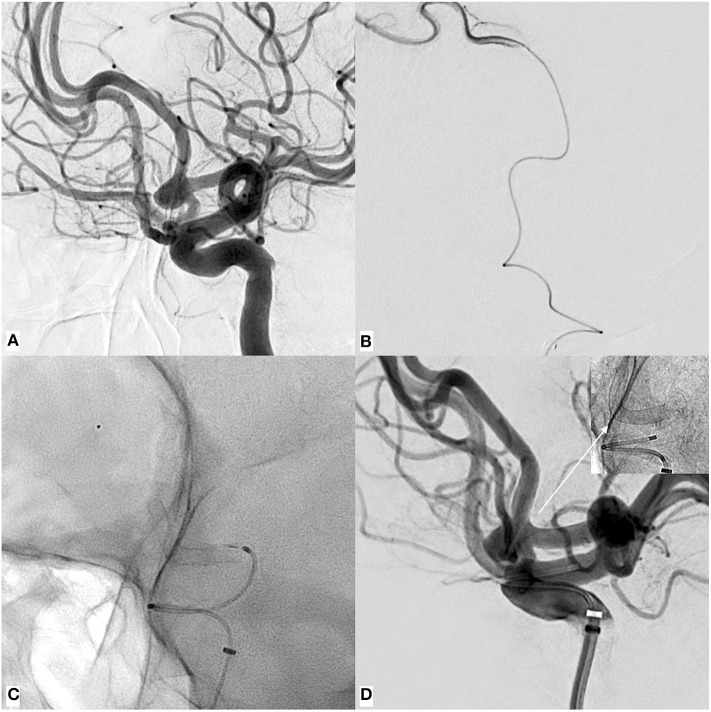
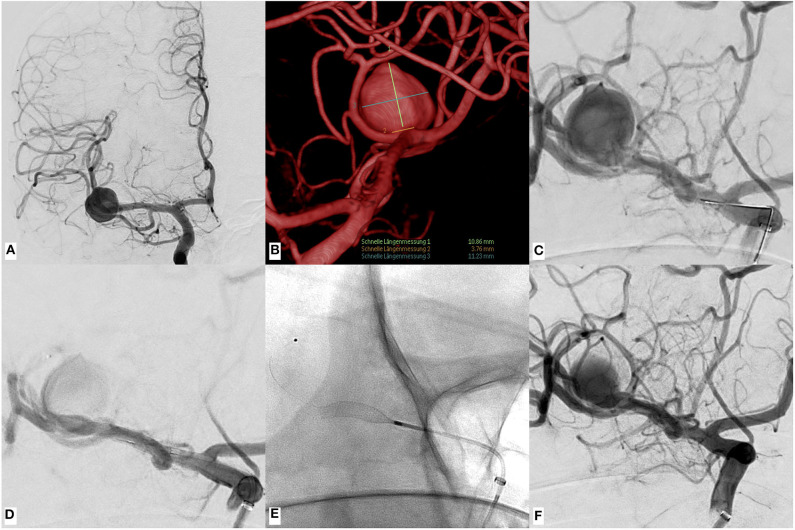
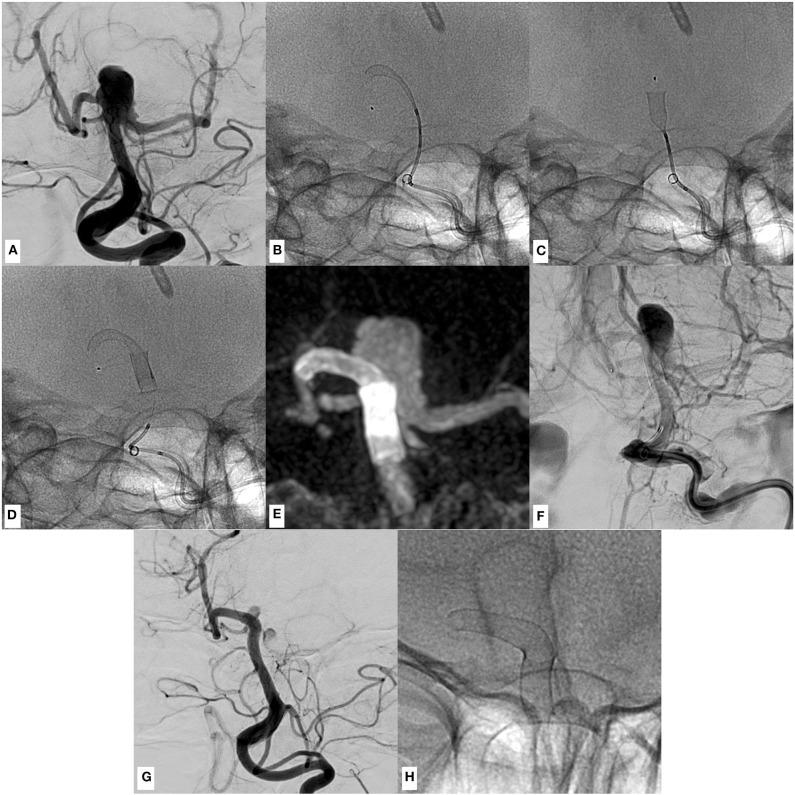
Background and Purpose: Flow diversion has profoundly changed the way aneurysms are treated. However, it conventionally requires dual antiplatelet medication and has yet been considered off-label use in the posterior circulation or within peripheral vessels of the anterior circulation. Here, we report our experience with the p48MW/p48MW hydrophilic coating (HPC) in the anterior and posterior circulation. This novel low-profile flow diverter is specifically designed for treatment of small peripheral vessels, and the p48MW HPC has an anti-thrombotic polymer coating, which allows application of a single antiplatelet function medication in conditions that expectably require further surgery. Materials and Methods: Thirty-two patients were prospectively included. Twenty-six treatments were performed with one flow diverter, four required two overlapping flow diverters, one case demanded three overlapping flow diverters, and in one case, extensive dissecting aneurysm telescoping with eight flow diverters was necessary. Twenty-two complex bifurcation aneurysms were treated. Three months' follow-up was available for 14 patients. Results: Deployment was uneventful in all cases. In four cases, undersizing was unavoidable and resulted in significant shortening of the flow diverter, which demanded implantation of further flow diverters to sufficiently treat the target aneurysm. Three flow diverters required balloon angioplasty for optimal wall approximation. All parent vessels remained patent. Available 3-month follow-up studies showed decreased influx or delayed washout in all aneurysms; none was occluded completely. There were no device-related clinical complications. Conclusions: Implantation of the p48MW/p48MW HPC is safe and effective for treatment of distally located cerebral aneurysms. Considering the reported rates of ischemic complications associated with flow diversion of complex bifurcation aneurysms, the p48MW/p48MW HPC potentially provides increased safety for complex bifurcation aneurysms in the anterior and posterior circulation.
Keywords: cerebral aneurysm; flow diversion; p48MW; reduced platelet function inhibition; small cerebral vessels.
Copyright © 2020 Schob, Kläver, Richter, Scherlach, Maybaum, Mucha, Schüngel, Hoffmann and Quaeschling.
Figures
References
-
- Colby GP, Bender MT, Lin LM, Beaty N, Caplan JM, Jiang B, et al. Declining complication rates with flow diversion of anterior circulation aneurysms after introduction of the Pipeline Flex: analysis of a single-institution series of 568 cases. J Neurosurg. (2018) 129:1475–81. 10.3171/2017.7.JNS171289 - DOI - PubMed
LinkOut - more resources
Full Text Sources