

Impact of Persistent Anemia on Systemic Inflammation and Tuberculosis Outcomes in Persons Living With HIV
- PMID: 33072136
- PMCID: PMC7541849
- DOI: 10.3389/fimmu.2020.588405
Impact of Persistent Anemia on Systemic Inflammation and Tuberculosis Outcomes in Persons Living With HIV
Abstract
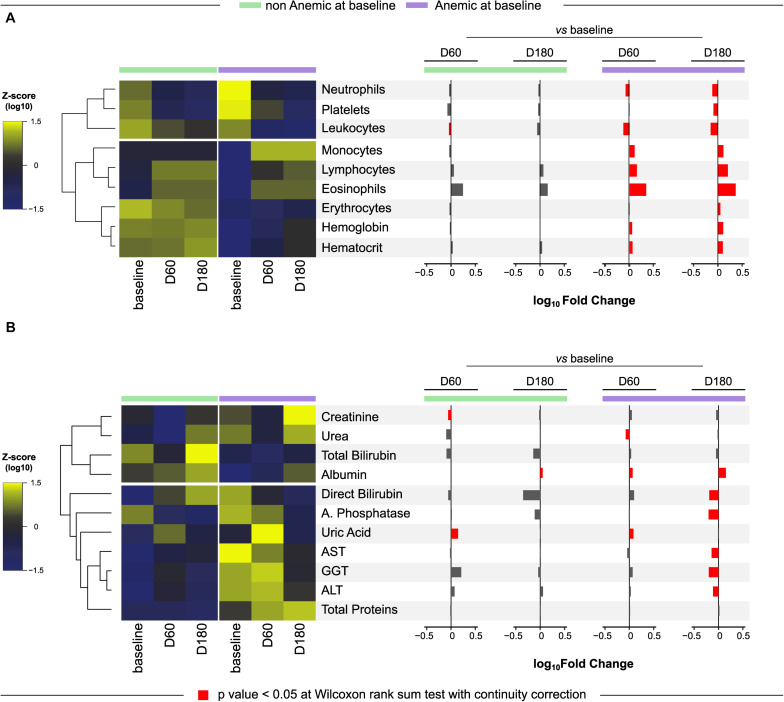
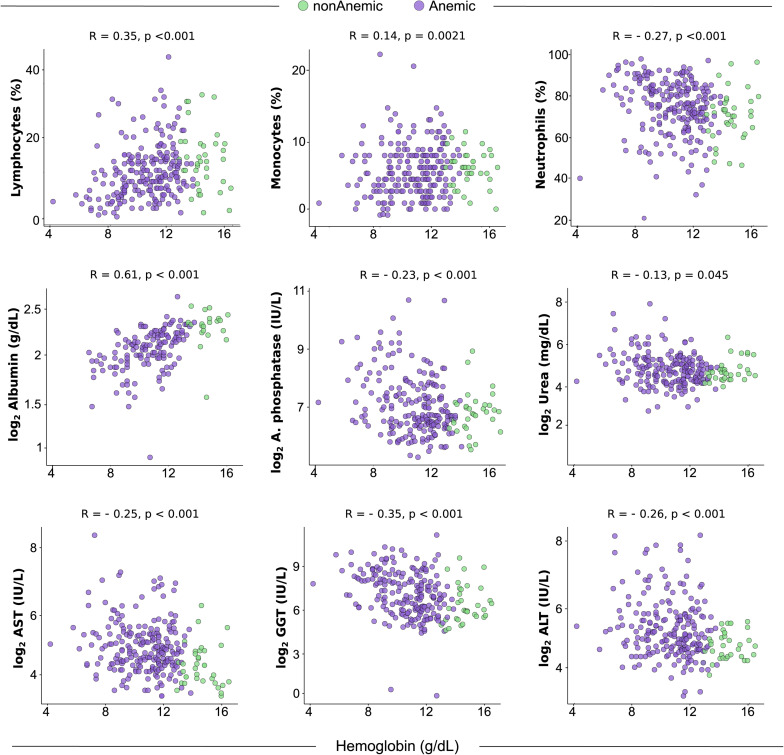
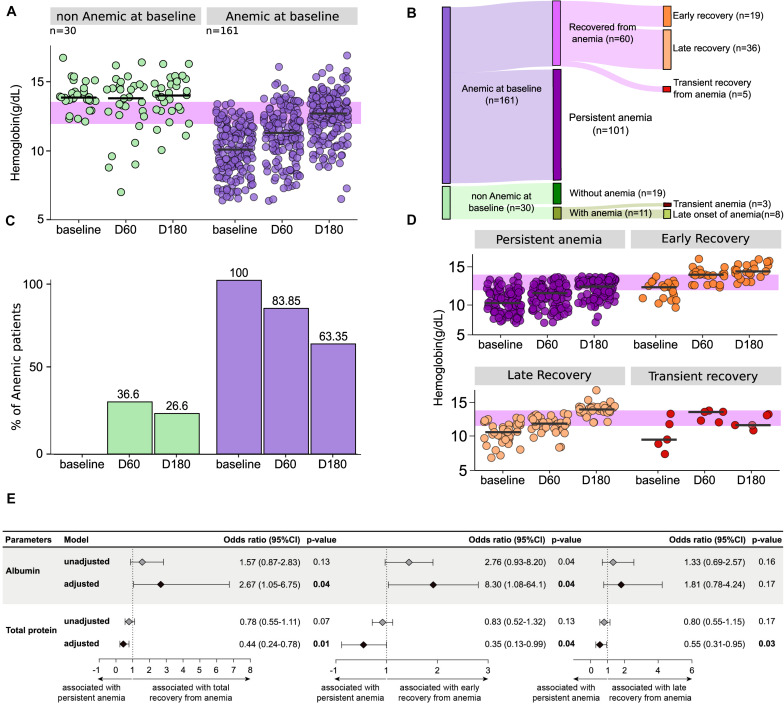
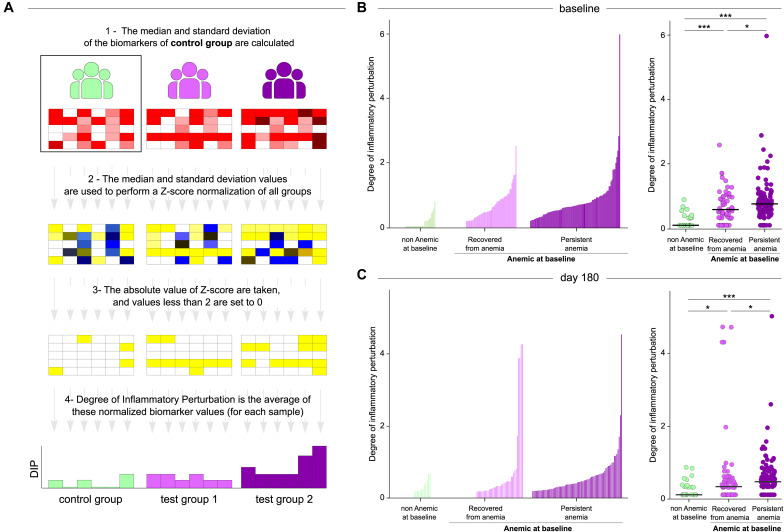
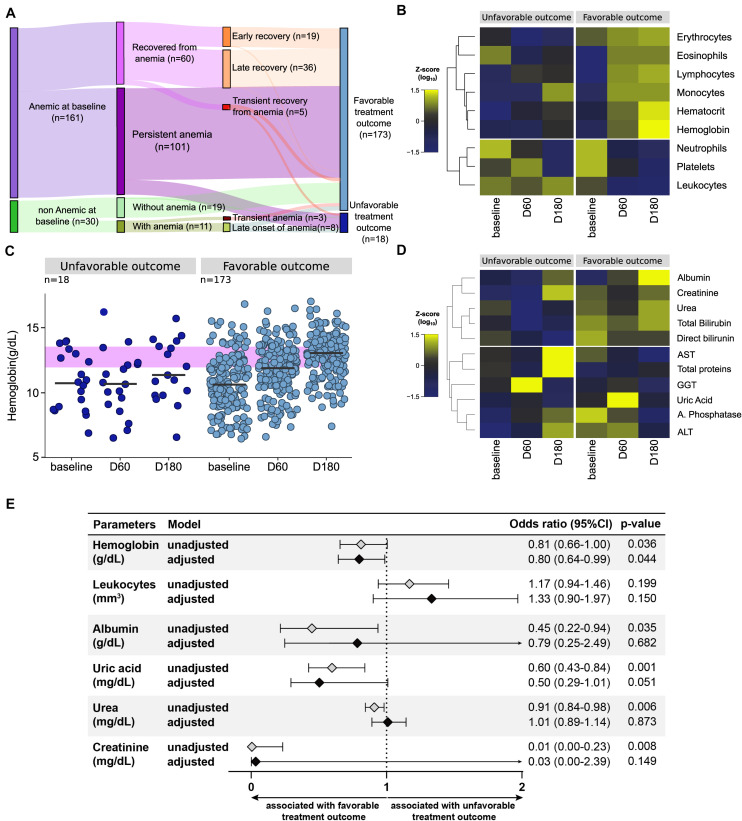
Tuberculosis (TB) is associated with systemic inflammation and anemia, which are aggravated in persons living with HIV (PLWH). Here, we characterized the dynamics of hemoglobin levels in PLWH coinfected with TB undergoing antitubercular therapy (ATT). We also examined the relationships between anemia and systemic inflammatory disturbance as well as the association between persistent anemia and unfavorable clinical outcomes. Data on several blood biochemical parameters and on blood cell counts were retrospectively analyzed in a cohort of 256 TB/HIV patients from Brazil during 180 days of ATT. Multidimensional statistical analyses were employed to profile systemic inflammation of patients stratified by anemia status (hemoglobin levels <12 g/dL for female and <13.5 g/dL for male individuals) prior to treatment and to perform prediction of unfavorable outcomes, such as treatment failure, loss to follow up and death. We found that 101 (63.63%) of patients with anemia at pre-ATT persisted with such condition until day 180. Such individuals exhibited heightened degree of inflammatory perturbation (DIP), which in turn was inversely correlated with hemoglobin levels. Recovery from anemia was associated with increased pre-ATT albumin levels whereas persistent anemia was related to higher total protein levels in serum. Multivariable regression analysis revealed that lower baseline hemoglobin levels was the major determinant of the unfavorable outcomes. Our findings demonstrate that persistent anemia in PLWH during the course of ATT is closely related with chronic inflammatory perturbation. Early intervention to promote recovery from anemia may improve ATT outcomes.
Keywords: HIV; anemia; inflammation; treatment outcome; tuberculosis.
Copyright © 2020 Demitto, Araújo-Pereira, Schmaltz, Sant’Anna, Arriaga, Andrade and Rolla.
Figures
References
-
- World Health Organization WHO Guidelines on Tuberculosis Infection Prevention and Control: 2019 Update. (2019). Available online at: http://www.ncbi.nlm.nih.gov/books/NBK539297/ (accessed July 27, 2020). - PubMed
-
- World Health Organization Fact Sheet Tuberculosis (TB). (2020). Available online at: https://www.who.int/news-room/fact-sheets/detail/tuberculosis (accessed July 27, 2020).
-
- World Health Organization Nutritional Anaemias: Tools for Effective Prevention and Control. Geneva: World Health Organization; (2017).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical