

Kinetics and isotype assessment of antibodies targeting the spike protein receptor-binding domain of severe acute respiratory syndrome-coronavirus-2 in COVID-19 patients as a function of age, biological sex and disease severity
- PMID: 33072323
- PMCID: PMC7541824
- DOI: 10.1002/cti2.1189
Kinetics and isotype assessment of antibodies targeting the spike protein receptor-binding domain of severe acute respiratory syndrome-coronavirus-2 in COVID-19 patients as a function of age, biological sex and disease severity
Abstract
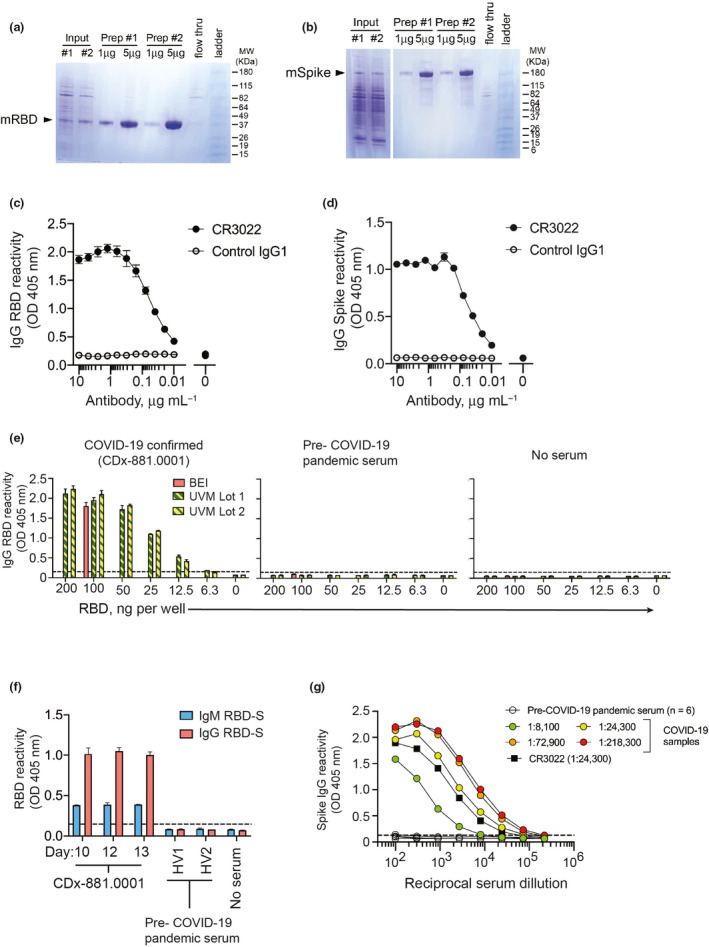
Objectives: There is an incomplete understanding of the host humoral immune response to severe acute respiratory syndrome (SARS)-coronavirus (CoV)-2, which underlies COVID-19, during acute infection. Host factors such as age and sex as well as the kinetics and functionality of antibody responses are important factors to consider as vaccine development proceeds. The receptor-binding domain of the CoV spike (RBD-S) protein mediates host cell binding and infection and is a major target for vaccine design to elicit neutralising antibodies.
Methods: We assessed serum anti-SARS-CoV-2 RBD-S IgG, IgM and IgA antibodies by a two-step ELISA and neutralising antibodies in a cross-sectional study of hospitalised COVID-19 patients of varying disease severities. Anti-RBD-S IgG levels were also determined in asymptomatic seropositives.
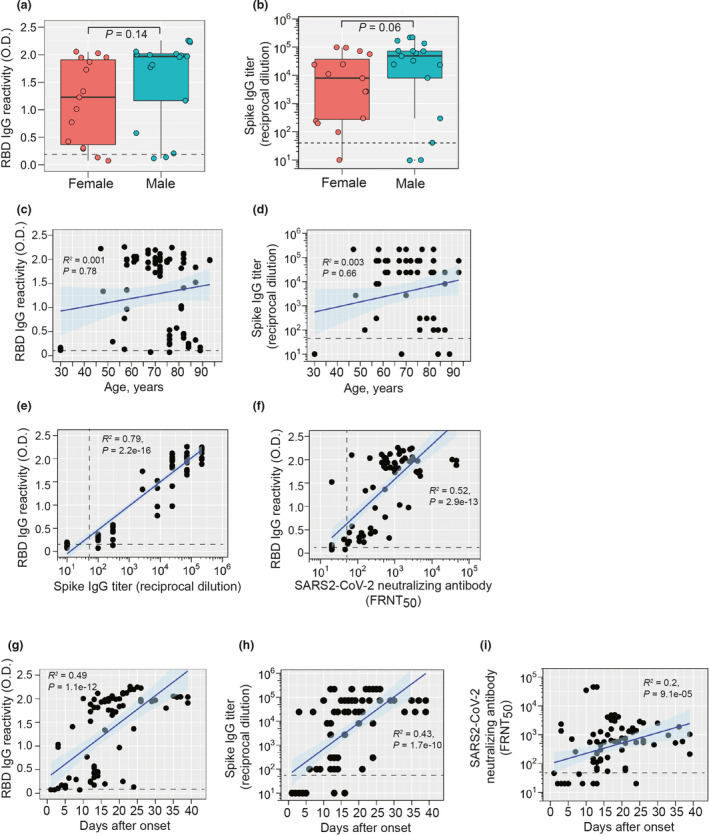
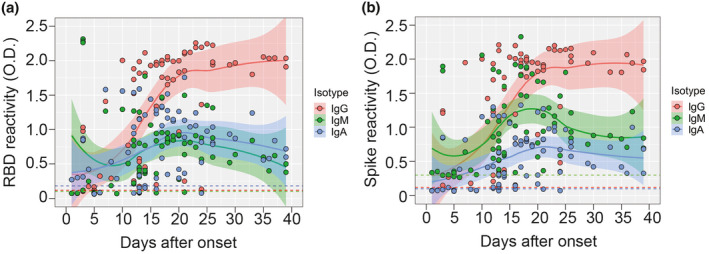
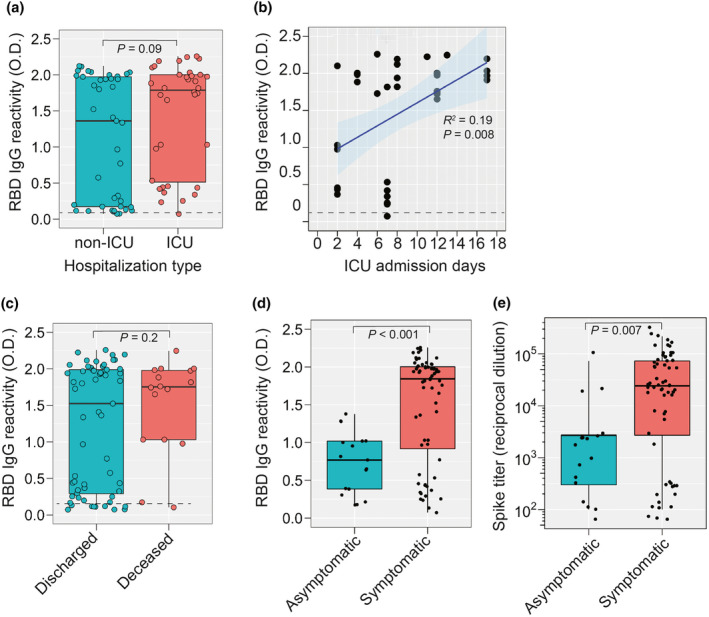
Results: We found equivalent levels of anti-RBD-S antibodies in male and female patients and no age-related deficiencies even out to 93 years of age. The anti-RBD-S response was evident as little as 6 days after onset of symptoms and for at least 5 weeks after symptom onset. Anti-RBD-S IgG, IgM and IgA responses were simultaneously induced within 10 days after onset, with anti-RBD-S IgG sustained over a 5-week period. Anti-RBD-S antibodies strongly correlated with neutralising activity. Lastly, anti-RBD-S IgG responses were higher in symptomatic COVID-19 patients during acute infection compared with asymptomatic seropositive donors.
Conclusion: Our results suggest that anti-RBD-S IgG reflect functional immune responses to SARS-CoV-2, but do not completely explain age- and sex-related disparities in COVID-19 fatalities.
Keywords: COVID‐19; SARS‐CoV‐2; humoral immune response; isotypes; neutralising antibody; spike protein.
© 2020 The Authors. Clinical & Translational Immunology published by John Wiley & Sons Australia, Ltd on behalf of Australian and New Zealand Society for Immunology, Inc.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Update of
-
Kinetics and Isotype Assessment of Antibodies Targeting the Spike Protein Receptor Binding Domain of SARS-CoV-2 In COVID-19 Patients as a function of Age and Biological Sex.medRxiv [Preprint]. 2020 Jul 16:2020.07.15.20154443. doi: 10.1101/2020.07.15.20154443. medRxiv. 2020. Update in: Clin Transl Immunology. 2020 Oct 07;9(10):e1189. doi: 10.1002/cti2.1189. PMID: 32743592 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous