

Early- and late anthracycline-induced cardiac dysfunction: echocardiographic characterization and response to heart failure therapy
- PMID: 33072403
- PMCID: PMC7557080
- DOI: 10.1186/s40959-020-00079-3
Early- and late anthracycline-induced cardiac dysfunction: echocardiographic characterization and response to heart failure therapy
Abstract
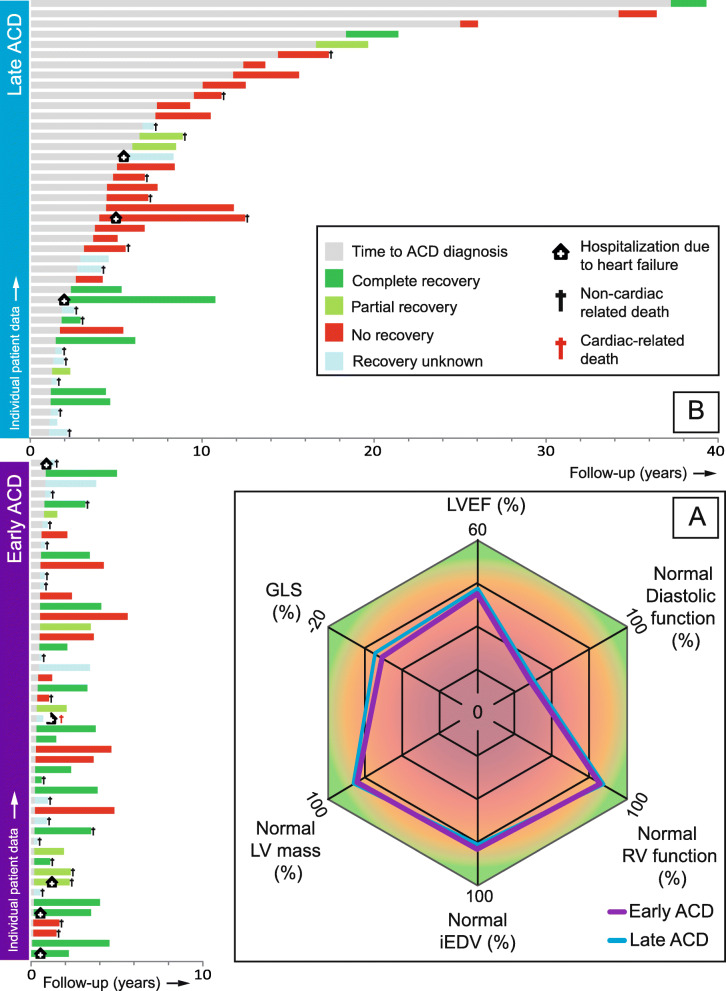
Background: Anthracycline-induced cardiac dysfunction (ACD) is a notorious side effect of anticancer treatment. It has been described as a phenomenon of a continuous progressive decline of cardiac function, eventually leading to dilated cardiomyopathy (DCM). This progressive nature suggests that patients with a delayed ACD diagnosis have greater compromise of cardiac function and more adverse remodeling, with a poor response to heart failure (HF) treatment. This study aimed to delineate the impact of a delayed ACD diagnosis on echocardiographic characteristics and response to HF treatment.
Methods and results: From the population of our cardio-oncology outpatient clinic, 92 ACD patients were included in this study (age 51.6 ± 16.2 years, median cumulative anthracycline dose 329 [200-329] mg/m2), and a median follow-up of 25.0 [9.6-37.2] months after ACD diagnosis. Median time to ACD diagnosis for patients diagnosed early (< 1 year) and late (> 1 year) was 4.0 vs. 47.7 months respectively. There were no echocardiographic differences between patients diagnosed early vs. late (LVEF 43.6 ± 4.9% vs. 43.0 ± 6.2% and iEDV 63.6 vs. 62.9 mL/m2). Eighty-three percent of patients presented with mild LV dysfunction and in 79% the LV was not dilated. Patients diagnosed early were more likely to have (partial) recovery of cardiac function upon HF treatment initiation (p = 0.015).
Conclusions: In the setting of a cardio-oncology outpatient clinic, patients with ACD presented with a hypokinetic non-dilated cardiomyopathy, rather than typical DCM. Timing of ACD diagnosis did not impact HF disease severity. However, in patients receiving an early diagnosis, cardiac function was more likely to recover upon HF treatment.
Keywords: Anthracyclines; Cardiac dysfunction; Cardiac effects of cancer treatment; Heart failure.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsNone declared.
Figures


References
-
- Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R, Galderisi M, et al. 2016 ESC position paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for practice guidelines: the task force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC) Eur Heart J. 2016;37(36):2768–2801. doi: 10.1093/eurheartj/ehw211. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous