

Subarachnoid Contrast Hyperdensity Following Pelvic Trauma Mimicking Diffuse Subarachnoid Hemorrhage
- PMID: 33072468
- PMCID: PMC7557717
- DOI: 10.7759/cureus.10460
Subarachnoid Contrast Hyperdensity Following Pelvic Trauma Mimicking Diffuse Subarachnoid Hemorrhage
Abstract
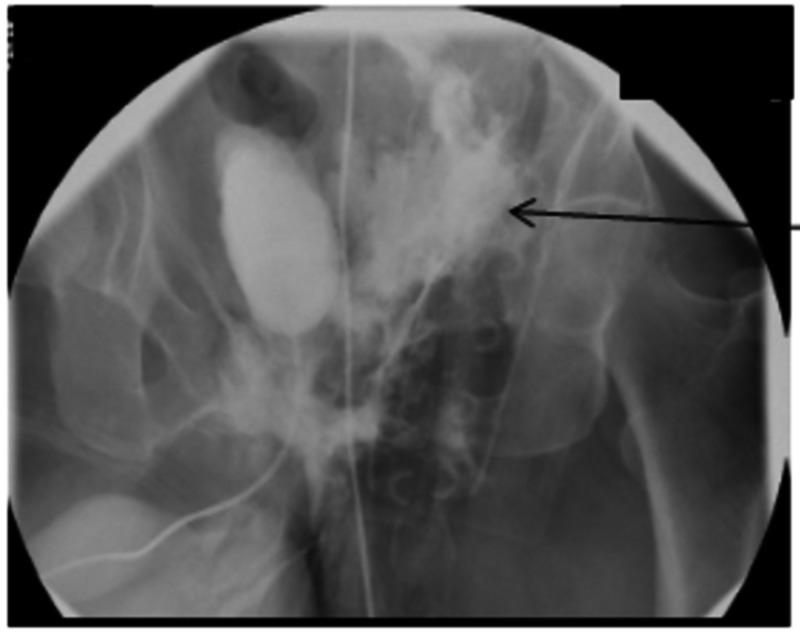
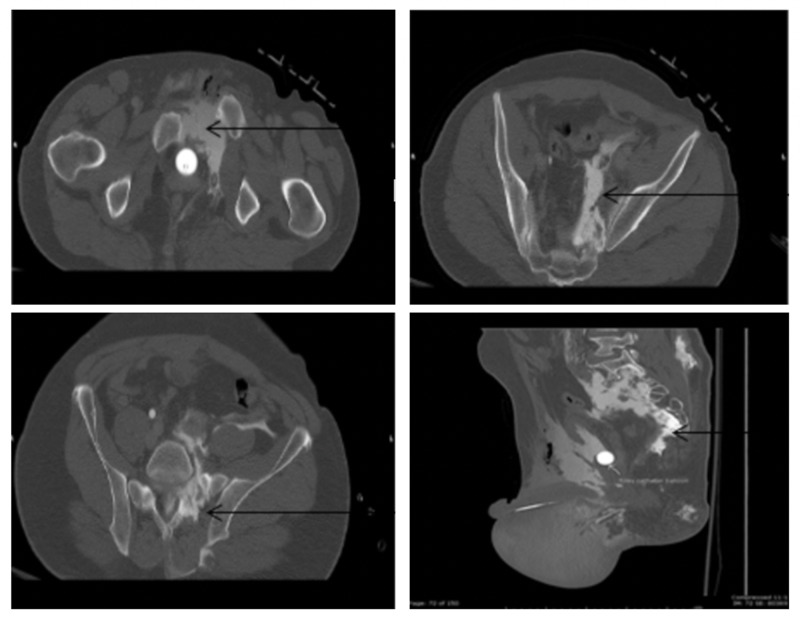
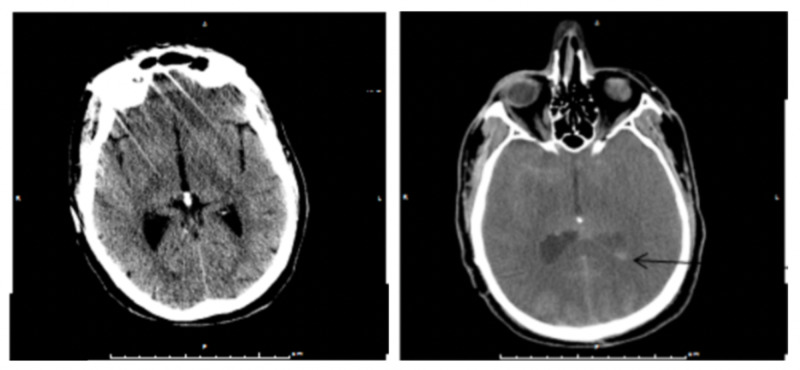
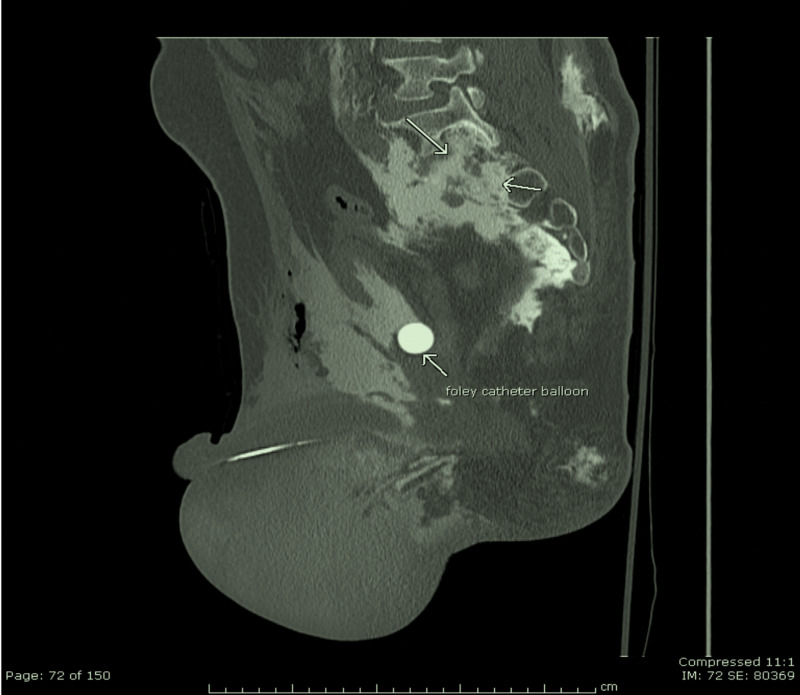
We present a case of a 54-year-old male who was involved in a motorcycle accident. His head computed tomography (CT) scan on arrival at our Level 1 institution was positive for hyperdensity suspicious for subarachnoid hemorrhage (SAH). Spine CT showed anterior compression fractures of T7-T9 vertebral bodies along with the presence of contrast within the subarachnoid space in the thoracic and lumbar spine, raising suspicion for a dural tear. CT of the chest, abdomen, and pelvis revealed open book pelvic fracture, left sacral ala fracture extending into the left sacroiliac joint and S1 neural foramen, coccygeal fracture, and extraperitoneal bladder rupture. This rare case report highlights the possibility of a spinal meningeal tear in severe pelvic trauma with concomitant bladder injury as a pathway of contrast entry into the normally impermeable cerebrospinal fluid (CSF) space mimicking traumatic subarachnoid hemorrhage.
Keywords: contrast hyperdensity; dural tear; pelvic trauma; subarachnoid hemorrhage.
Copyright © 2020, Biswas et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Traumatic Cervical Vertebral Artery Transection Associated with a Dural Tear Leading to Subarachnoid Extravasation.Eur J Trauma Emerg Surg. 2009 Feb;35(1):67-70. doi: 10.1007/s00068-008-7184-z. Epub 2008 Jul 17. Eur J Trauma Emerg Surg. 2009. PMID: 26814535
-
[Spiral computed tomography in the assessment of vascular lesions of the pelvis due to blunt trauma].Radiol Med. 2000 Jul-Aug;100(1-2):29-32. Radiol Med. 2000. PMID: 11109448 Italian.
-
Intracranial transthecal subarachnoid fat emboli and subarachnoid haemorrhage arising from a sacral fracture and dural tear.Br J Radiol. 2010 Jan;83(985):e18-21. doi: 10.1259/bjr/66268641. Br J Radiol. 2010. PMID: 20139244 Free PMC article.
-
Supratentorial subdural hemorrhage of a previous head injury and cerebellar hemorrhage after cervical spinal surgery: a case report and review of the literature.Spine (Phila Pa 1976). 2014 May 20;39(12):E743-7. doi: 10.1097/BRS.0000000000000323. Spine (Phila Pa 1976). 2014. PMID: 24718071 Review.
-
[Subdural hematoma at the cranio-vertebral junction following head trauma: a case report].No Shinkei Geka. 2010 Apr;38(4):365-70. No Shinkei Geka. 2010. PMID: 20387579 Review. Japanese.
References
-
- Pseudo-subarachnoid hemorrhage: a rare neuroimaging pitfall. Al-Yamany M, Deck J, Bernstein M. https://pubmed.ncbi.nlm.nih.gov/10068810/ Can J Neuro Sci. 1999;26:57–59. - PubMed
-
- Pseudo-subarachnoid hemorrhage: a potential imaging pitfall associated with diffuse cerebral edema. Given CA 2nd, Burdette JH, Elster AD, Williams DW 3rd. https://pubmed.ncbi.nlm.nih.gov/12591643/ AJNR Am J Neuroradiol. 2003;24:254–256. - PMC - PubMed
-
- Acute purulent leptomeningitis mimicking subarachnoid hemorrhage on CT. Mendelsohn DB, Moss ML, Chason DP, Muphree S, Casey S. J Comput Assist Tomogr. 1994;18:126–128. - PubMed
-
- Increased density of tentorium and falx: a false positive CT sign of subarachnoid hemorrhage. Spiegel SM, Fox AJ, Vinuela F, Pelz DM. https://pubmed.ncbi.nlm.nih.gov/2950107/ Can Assoc Radiol J. 1986;37:243–247. - PubMed
-
- The false falx sign. Osborn AG, Anderson RE, Wing DS. Radiology. 1980;134:421–425. - PubMed
Publication types
LinkOut - more resources
Full Text Sources