

Comparison of Current Systemic Combination Therapies for Metastatic Hormone-Sensitive Prostate Cancer and Selection of Candidates for Optimal Treatment: A Systematic Review and Bayesian Network Meta-Analysis
- PMID: 33072564
- PMCID: PMC7531177
- DOI: 10.3389/fonc.2020.519388
Comparison of Current Systemic Combination Therapies for Metastatic Hormone-Sensitive Prostate Cancer and Selection of Candidates for Optimal Treatment: A Systematic Review and Bayesian Network Meta-Analysis
Abstract
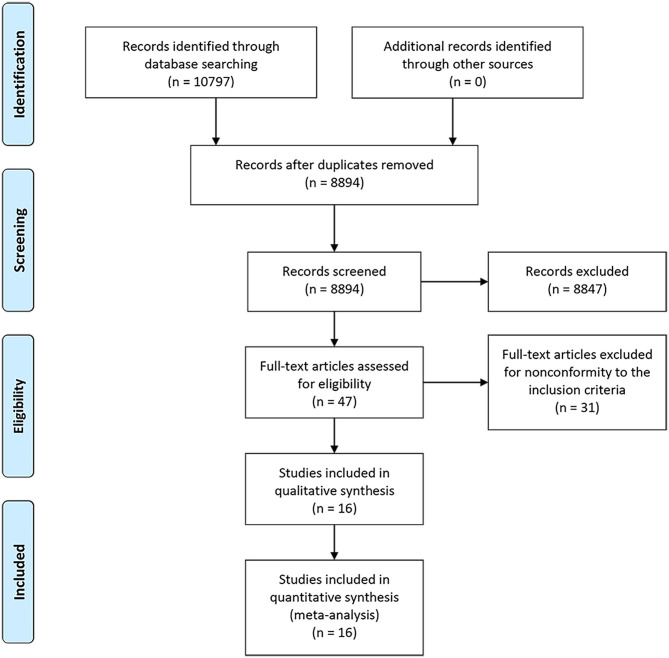
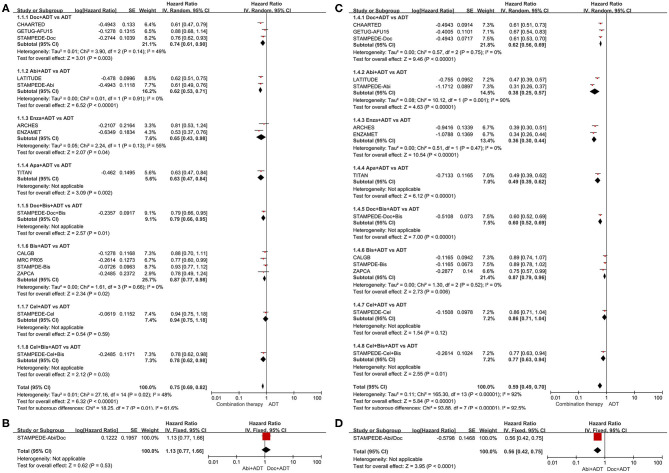
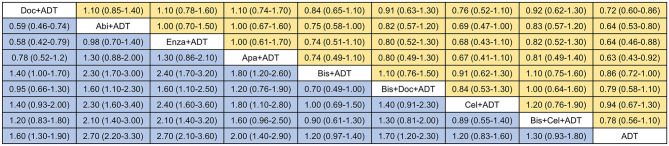
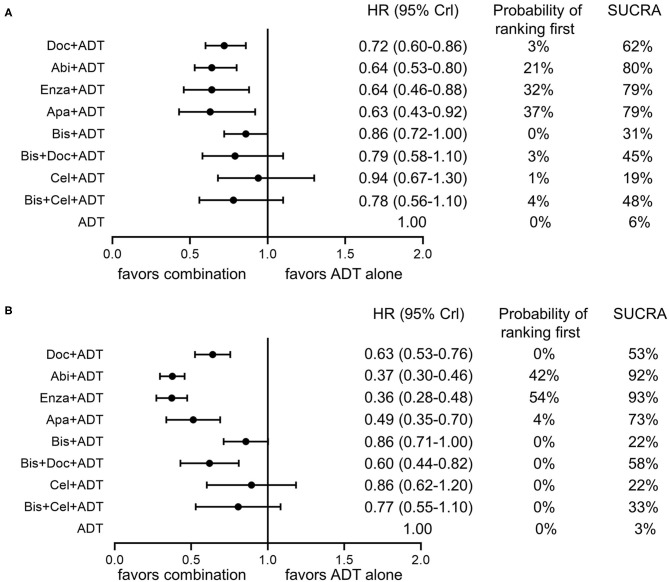
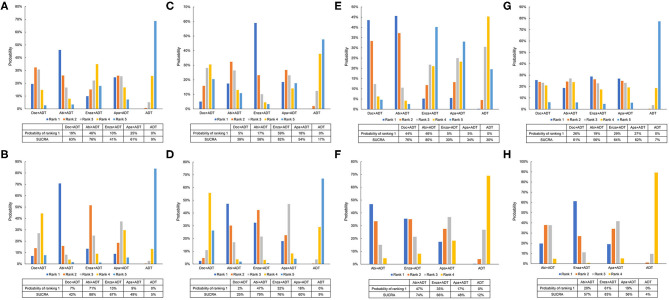
Objective: To compare the efficacy and safety of current systemic combination therapies for patients with mHSPC and help select candidates for optimal treatment. Methods: Databases of MEDLINE and EMBASE, Cochrane Central Register of Controlled Trials, and Clinical Trial.gov were searched for eligible studies. Direct and network meta-analysis were conducted to compare various systemic combination therapies and the surface under the cumulative ranking curve (SUCRA) was generated for treatment ranking. Subgroup analyses were performed according to the extent of metastasis. Adverse events (AEs) were compared among the effective treatments. Results: Ten trials with 16 publications were included in this network meta-analysis. Direct and network meta-analysis consistently suggested that androgen-deprivation therapy (ADT) combined with docetaxel, abiraterone, enzalutamide, or apalutamide could significantly improve overall survival (OS) and failure-free survival (FFS) compared to ADT alone in men with mHSPC. SUCRA analysis demonstrated the superiority of ADT plus abiraterone or enzalutamide over other therapies. Subgroup analyses indicated that additional abiraterone to ADT had the highest ranking in patients with high-volume diseases or visceral metastases and enzalutamide plus ADT outperformed other treatments in patients with low-volume diseases or without visceral metastases. Different combination therapies had variable AE profiles and ADT in addition with docetaxel or abiraterone had the highest risk of AEs. Conclusion: ADT plus docetaxel, abiraterone, enzalutamide, or apalutamide were associated with significantly improved survival in patients with mHSPC. ADT plus abiraterone or enzalutamide appeared to be the most effective treatments. Clinicians should balance the efficacy, potential AEs, and disease status to select the optimal treatment.
Keywords: androgen-deprivation therapy; chemotherapy; combination therapy; metastatic prostate cancer; network meta-analysis.
Copyright © 2020 Chen, Ni, Sun, Liao, Zhang, Zhao, Zhu, Wang, Shen and Zeng.
Figures
References
-
- Dearnaley DP, Mason MD, Parmar MKB, Sanders K, Sydes MR. Adjuvant therapy with oral sodium clodronate in locally advanced and metastatic prostate cancer: long-term overall survival results from the MRC PR04 and PR05 randomised controlled trials. Lancet Oncol. (2009) 10:872–6. 10.1016/S1470-2045(09)70201-3 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources