

Biomarkers and antithrombotic treatment in cervical artery dissection - Design of the TREAT-CAD randomised trial
- PMID: 33072885
- PMCID: PMC7538765
- DOI: 10.1177/2396987320921151
Biomarkers and antithrombotic treatment in cervical artery dissection - Design of the TREAT-CAD randomised trial
Abstract
Introduction: The type of antithrombotic treatment in cervical artery dissection patients is still a matter of debate. Most physicians prefer anticoagulants over antiplatelet agents for stroke prevention. However, this approach is not evidence-based and antiplatelets might be as safe and as effective. The 'Biomarkers and Antithrombotic Treatment in Cervical Artery Dissection' ('TREAT-CAD') trial (clinicaltrials.gov: NCT02046460) compares Aspirin to oral anticoagulants (vitamin K antagonists) with regard to efficacy and safety by using both clinical and imaging surrogate outcome measures. TREAT-CAD tests the hypothesis, that aspirin is as safe and effective as vitamin K antagonists.
Patients and methods: TREAD-CAD is a Prospective, Randomised controlled, Open-labelled, multicentre, non-inferiority trial with Blinded assessment of outcome Events (PROBE-design). Key eligibility criteria are (i) clinical symptoms attributable to cervical artery dissection and (ii) verification of the cervical artery dissection diagnosis by established magnetic resonance imaging criteria. Patients are randomised to receive either Aspirin 300 mg daily or vitamin K antagonists for 90 days.
Results: Primary outcomes are assessed at 14 ± 10 days (magnetic resonance imaging and clinical examination) and at 90 ± 30 days (clinical examinations). The primary endpoint is a composite outcome measure - labelled Cerebrovascular Ischemia, major Hemorrhagic events or Death (CIHD) - and includes (i) occurrence of any stroke (including retinal infarction), (ii) new ischaemic lesions on diffusion-weighted magnetic resonance imaging, (iii) any major extracranial haemorrhage, (iv) any symptomatic intracranial haemorrhage, (v) any new haemorrhagic lesion visible on paramagnetic-susceptible sequences and (vi) death.
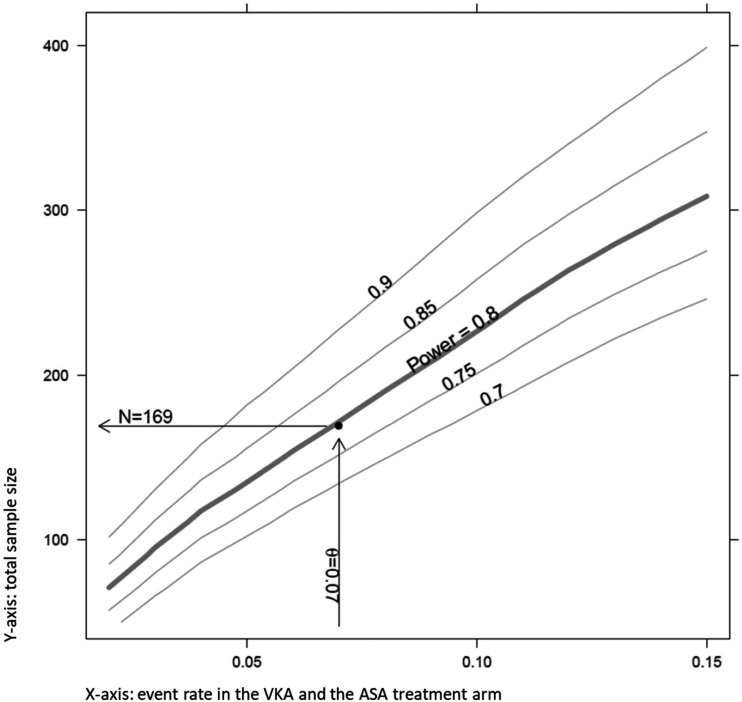
Discussion: After database closure, (i) central verification of cervical artery dissection diagnosis will be done by two experienced raters, (ii) adjudication of outcome events will be performed by independent adjudication committees, separately for clinical and imaging outcomes. The primary analysis will be done on the per protocol data set. The targeted sample size consists of 169 evaluable patients in the per protocol data set.
Conclusion: TREAT-CAD is testing the non-inferiority of Aspirin versus vitamin K antagonists treatment in patients with symptomatic cervical artery dissection by combined clinical and magnetic resonance imaging outcomes.
Keywords: Cervical artery dissection; anticoagulants; antiplatelets; prevention; randomised clinical trial; stroke.
© European Stroke Organisation 2020.
Figures

Similar articles
-
The 6-months follow-up of the TREAT-CAD trial: Aspirin versus anticoagulation for stroke prevention in patients with cervical artery dissection.Eur Stroke J. 2025 Feb 5:23969873251315362. doi: 10.1177/23969873251315362. Online ahead of print. Eur Stroke J. 2025. PMID: 39910883 Free PMC article.
-
Aspirin versus anticoagulation in cervical artery dissection (TREAT-CAD): an open-label, randomised, non-inferiority trial.Lancet Neurol. 2021 May;20(5):341-350. doi: 10.1016/S1474-4422(21)00044-2. Epub 2021 Mar 23. Lancet Neurol. 2021. PMID: 33765420 Clinical Trial.
-
Antithrombotic Treatment for Cervical Artery Dissection: A Systematic Review and Individual Patient Data Meta-Analysis.JAMA Neurol. 2024 Jun 1;81(6):630-637. doi: 10.1001/jamaneurol.2024.1141. JAMA Neurol. 2024. PMID: 38739383 Free PMC article.
-
New ischaemic brain lesions in cervical artery dissection stratified to antiplatelets or anticoagulants.Eur J Neurol. 2015 May;22(5):859-65, e61. doi: 10.1111/ene.12682. Epub 2015 Feb 24. Eur J Neurol. 2015. PMID: 25712171
-
Stroke Prevention in Cervical Artery Dissection.Curr Cardiol Rep. 2021 Oct 23;23(12):182. doi: 10.1007/s11886-021-01603-2. Curr Cardiol Rep. 2021. PMID: 34687376 Review.
Cited by
-
ESO guideline for the management of extracranial and intracranial artery dissection.Eur Stroke J. 2021 Sep;6(3):XXXIX-LXXXVIII. doi: 10.1177/23969873211046475. Epub 2021 Oct 13. Eur Stroke J. 2021. PMID: 34746432 Free PMC article.
-
Antithrombotic drugs for carotid artery dissection: Updated systematic review.Eur Stroke J. 2025 Jun;10(2):339-349. doi: 10.1177/23969873241292278. Epub 2024 Oct 26. Eur Stroke J. 2025. PMID: 39460559 Free PMC article.
-
Surgical and radiological interventions for treating symptomatic extracranial cervical artery dissection.Cochrane Database Syst Rev. 2021 Feb 1;2(2):CD013118. doi: 10.1002/14651858.CD013118.pub2. Cochrane Database Syst Rev. 2021. PMID: 34559418 Free PMC article.
-
The 6-months follow-up of the TREAT-CAD trial: Aspirin versus anticoagulation for stroke prevention in patients with cervical artery dissection.Eur Stroke J. 2025 Feb 5:23969873251315362. doi: 10.1177/23969873251315362. Online ahead of print. Eur Stroke J. 2025. PMID: 39910883 Free PMC article.
-
Management of cervical artery dissection: new evidence and future directions.J Neurol. 2025 May 27;272(6):426. doi: 10.1007/s00415-025-13166-1. J Neurol. 2025. PMID: 40423824 Free PMC article. Review.
References
-
- Debette S, Leys D. Cervical-artery dissections: predisposing factors, diagnosis, and outcome. Lancet Neurol 2009; 8: 668–678. - PubMed
-
- Engelter ST, Traenka C, Lyrer P. Dissection of Cervical and Cerebral Arteries. Curr Neurol Neurosci Rep 2017; 17: 59. - PubMed
-
- Menon RK, Markus HS, Norris JW. Results of a UK questionnaire of diagnosis and treatment in cervical artery dissection. J Neurol Neurosurg Psychiatry 2008; 79: 612. - PubMed
-
- Menon R, Kerry S, Norris JW, et al. Treatment of cervical artery dissection: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry 2008; 79: 1122–1127. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
