

Liver Metastases of Intrahepatic Cholangiocarcinoma: Implications for an Updated Staging System
- PMID: 33073396
- PMCID: PMC8252018
- DOI: 10.1002/hep.31598
Liver Metastases of Intrahepatic Cholangiocarcinoma: Implications for an Updated Staging System
Abstract
Background and aims: Intrahepatic cholangiocarcinoma (iCCA) with liver metastases is perceived to have a poor prognosis, but the American Joint Committee on Cancer (AJCC) classifies them as early stage in the absence of lymph nodes or extrahepatic spread.
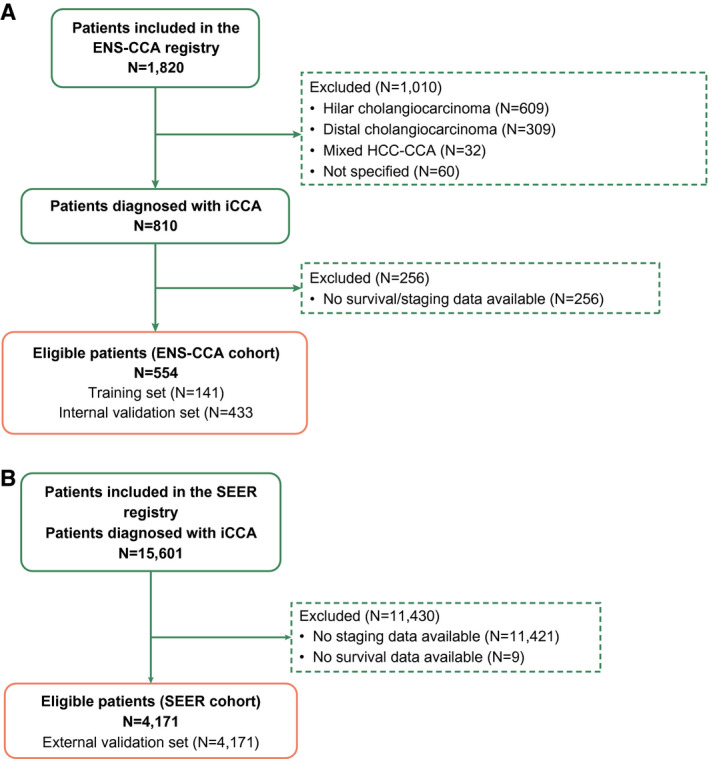
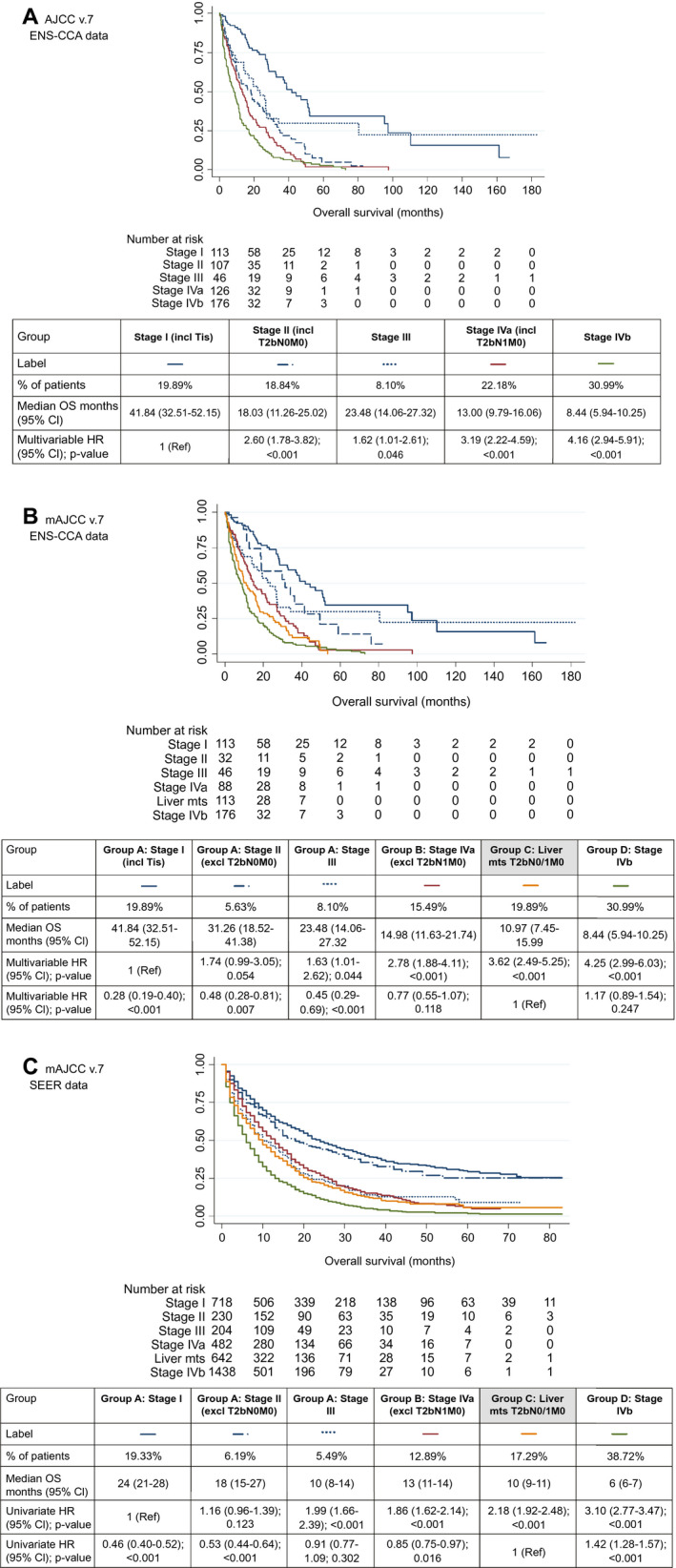
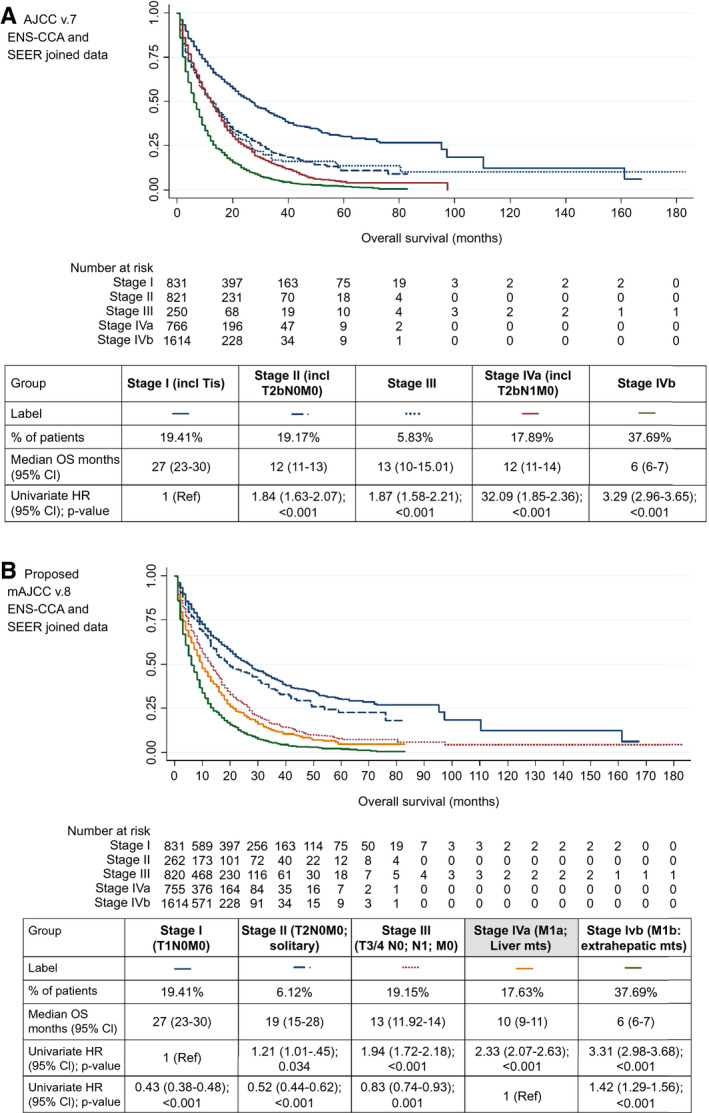
Approach and results: Patients with iCCA from the European Network for the Study of Cholangiocarcinoma (ENS-CCA) and Surveillance, Epidemiology, and End Results (SEER) registries with survival/staging (AJCC v.7) data were eligible. Modified staging was used (mAJCC v.7): group A: stages I-III (excluding T2bN0); group B: stage IVa (excluding T2bN1M0); group C: liver metastases (T2bN0/1); and group D: stage IVb (extrahepatic metastases). Survival analysis (Kaplan-Meier and Cox regression) was performed in an ENS-CCA training cohort (TC) and findings internally (ENS-CCA iVC) and externally (SEER) validated. The aim was to assess whether liver metastases (group C) had a shorter survival compared to other early stages (group A) to propose a modified version of AJCC v.8 (mAJCC v.8). A total of 574 and 4,171 patients from the ENS-CCA and SEER registries were included. Following the new classification, 19.86% and 17.31% of patients from the ENS-CCA and SEER registries were reclassified into group C, respectively. In the ENS-CCA TC, multivariable Cox regression was adjusted for obesity (p = 0.026) and performance status (P < 0.001); patients in group C (HR, 2.53; 95% CI, 1.18-5.42; P = 0.017) had a higher risk of death (vs. group A). Findings were validated in the ENS-CCA iVC (HR, 2.93; 95% CI, 2.04-4.19; P < 0.001) and in the SEER registry (HR, 1.88; 95% CI, 1.68-2.09; P < 0.001).
Conclusions: iCCA with liver metastases has a worse outcome than other early stages of iCCA. Given that AJCC v.8 does not take this into consideration, a modification of AJCC v.8 (mAJCC v.8), including "liver metastases: multiple liver lesions, with or without vascular invasion" as an "M1a stage," is suggested.
© 2020 The Authors. Hepatology published by Wiley Periodicals LLC on behalf of American Association for the Study of Liver Diseases.
Figures
Comment in
-
Letter to the Editor: Does Multiple Intrahepatic Cholangiocarcinoma Worsen Prognosis as "M1" Stage?Hepatology. 2021 Aug;74(2):1128. doi: 10.1002/hep.31741. Epub 2021 Jun 18. Hepatology. 2021. PMID: 33550583 No abstract available.
-
REPLY.Hepatology. 2021 Aug;74(2):1129-1131. doi: 10.1002/hep.31740. Epub 2021 Aug 10. Hepatology. 2021. PMID: 33550618 No abstract available.
-
REPLY.Hepatology. 2021 Oct;74(4):2319-2321. doi: 10.1002/hep.31904. Epub 2021 Aug 21. Hepatology. 2021. PMID: 33998692 No abstract available.
-
Letter to the Editor: The Role of Surgery in Multiple Intrahepatic Cholangiocarcinoma Should Not Be Dismissed Without Further Analysis.Hepatology. 2021 Oct;74(4):2318-2319. doi: 10.1002/hep.31905. Epub 2021 Aug 22. Hepatology. 2021. PMID: 34002414 No abstract available.
References
-
- Patel T. Increasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United States. Hepatology 2001;33:1353‐1357. - PubMed
-
- Anderson C, Kim R. Adjuvant therapy for resected extrahepatic cholangiocarcinoma: a review of the literature and future directions. Cancer Treat Rev 2009;35:322‐327. - PubMed
-
- Banales JM, Cardinale V, Carpino G, et al. Expert consensus document: cholangiocarcinoma: current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS‐CCA). Nat Rev Gastroenterol Hepatol 2016;13:261‐280. - PubMed
-
- Lamarca A, Frizziero M, McNamara MG, Valle JW. Clinical and translational research challenges in biliary tract cancers. Curr Med Chem 2020;27:4756‐4777. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
