

Primary Results From the Understanding Outcomes With the S-ICD in Primary Prevention Patients With Low Ejection Fraction (UNTOUCHED) Trial
- PMID: 33073614
- PMCID: PMC7752215
- DOI: 10.1161/CIRCULATIONAHA.120.048728
Primary Results From the Understanding Outcomes With the S-ICD in Primary Prevention Patients With Low Ejection Fraction (UNTOUCHED) Trial
Abstract
Background: The subcutaneous (S) implantable cardioverter-defibrillator (ICD) is safe and effective for sudden cardiac death prevention. However, patients in previous S-ICD studies had fewer comorbidities, had less left ventricular dysfunction, and received more inappropriate shocks (IAS) than in typical transvenous ICD trials. The UNTOUCHED trial (Understanding Outcomes With the S-ICD in Primary Prevention Patients With Low Ejection Fraction) was designed to evaluate the IAS rate in a more typical, contemporary ICD patient population implanted with the S-ICD using standardized programming and enhanced discrimination algorithms.
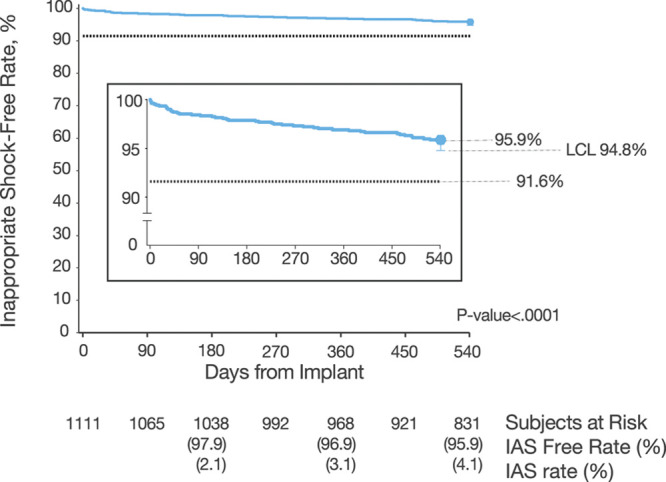
Methods: Primary prevention patients with left ventricular ejection fraction ≤35% and no pacing indications were included. Generation 2 or 3 S-ICD devices were implanted and programmed with rate-based therapy delivery for rates ≥250 beats per minute and morphology discrimination for rates ≥200 and <250 beats per minute. Patients were followed for 18 months. The primary end point was the IAS-free rate compared with a 91.6% performance goal, derived from the results for the ICD-only patients in the MADIT-RIT study (Multicenter Automatic Defibrillator Implantation Trial-Reduce Inappropriate Therapy). Kaplan-Meier analyses were performed to evaluate event-free rates for IAS, all-cause shock, and complications. Multivariable proportional hazard analysis was performed to determine predictors of end points.
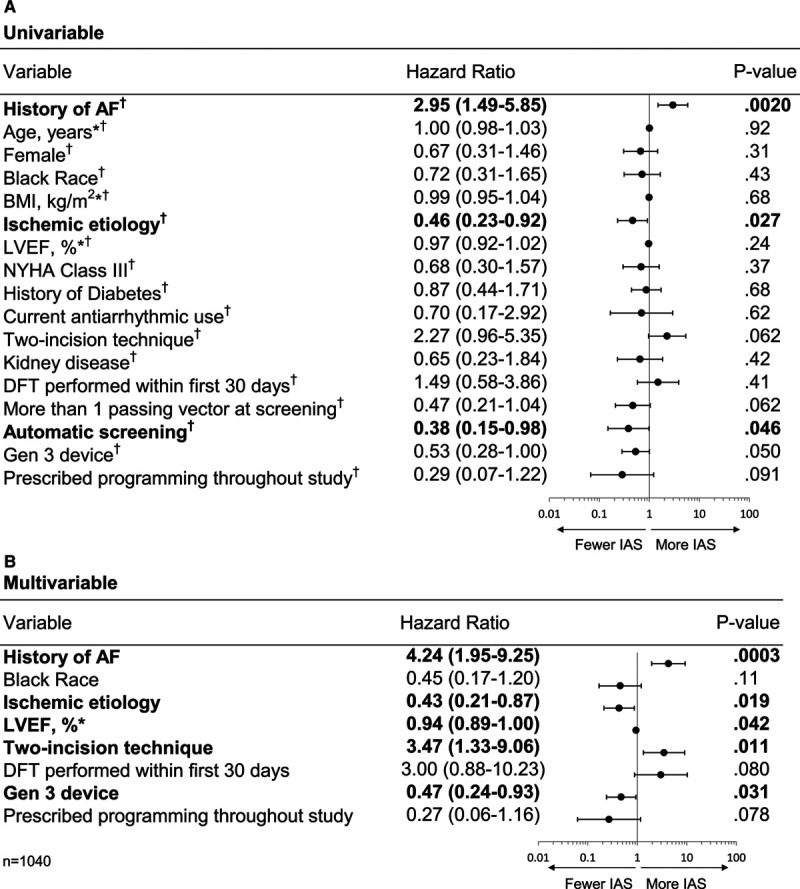
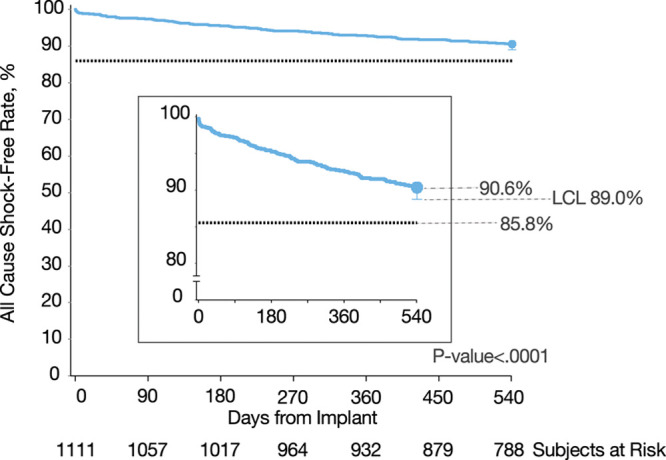
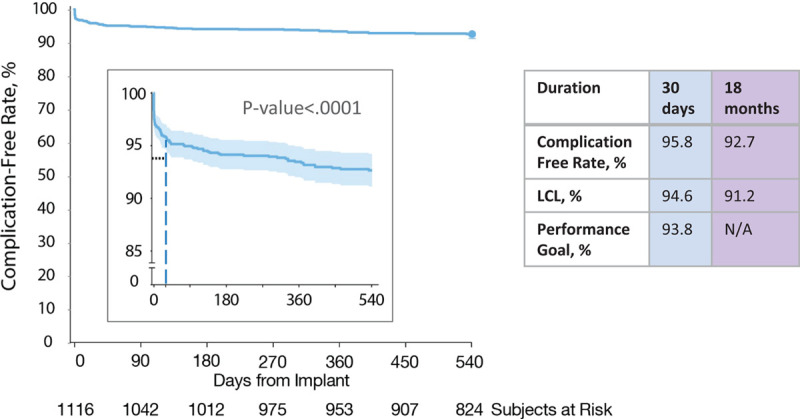
Results: S-ICD implant was attempted in 1116 patients, and 1111 patients were included in postimplant follow-up analysis. The cohort had a mean age of 55.8±12.4 years, 25.6% were women, 23.4% were Black, 53.5% had ischemic heart disease, 87.7% had symptomatic heart failure, and the mean left ventricular ejection fraction was 26.4±5.8%. Eighteen-month freedom from IAS was 95.9% (lower confidence limit, 94.8%). Predictors of reduced incidence of IAS were implanting the most recent generation of device, using the 3-incision technique, no history of atrial fibrillation, and ischemic cause. The 18-month all-cause shock-free rate was 90.6% (lower confidence limit, 89.0%), meeting the prespecified performance goal of 85.8%. Conversion success rate for appropriate, discrete episodes was 98.4%. Complication-free rate at 18 months was 92.7%.
Conclusions: This study demonstrates high efficacy and safety with contemporary S-ICD devices and programming despite the relatively high incidence of comorbidities in comparison with earlier S-ICD trials. The inappropriate shock rate (3.1% at 1 year) is the lowest reported for the S-ICD and lower than many transvenous ICD studies using contemporary programming to reduce IAS. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT02433379.
Keywords: arrhythmias, cardiac; defibrillators, implantable; heart failure; primary prevention; sudden cardiac death; ventricular fibrillation; ventricular tachycardia.
Figures
Comment in
-
Be-All End-All Real-World Evidence on the Subcutaneous ICD.Circulation. 2021 Jan 5;143(1):18-20. doi: 10.1161/CIRCULATIONAHA.120.050861. Epub 2020 Dec 30. Circulation. 2021. PMID: 33378236 No abstract available.
References
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, et al. Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–237. doi: 10.1056/NEJMoa043399 - PubMed
-
- Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N Engl J Med. 1999;341:1882–1890. doi: 10.1056/NEJM199912163412503 - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H, Levine JH, Saksena S, Waldo AL, Wilber D, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N Engl J Med. 1996;335:1933–1940. doi: 10.1056/NEJM199612263352601 - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, Daubert JP, Higgins SL, Brown MW, Andrews ML. Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–883. doi: 10.1056/NEJMoa013474 - PubMed
-
- Zipes DP, Wyse DG, Friedman PL, Epstein AE, Hallstrom AP, Greene HL, Schron EB, Domanski M. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. N Engl J Med. 1997;337:1576–1583. doi: 10.1056/NEJM199711273372202 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
