

Association of Bevacizumab Plus Oxaliplatin-Based Chemotherapy With Disease-Free Survival and Overall Survival in Patients With Stage II Colon Cancer: A Secondary Analysis of the AVANT Trial
- PMID: 33074326
- PMCID: PMC7573695
- DOI: 10.1001/jamanetworkopen.2020.20425
Association of Bevacizumab Plus Oxaliplatin-Based Chemotherapy With Disease-Free Survival and Overall Survival in Patients With Stage II Colon Cancer: A Secondary Analysis of the AVANT Trial
Erratum in
-
Errors in Abstract and Figure.JAMA Netw Open. 2021 Feb 1;4(2):e210700. doi: 10.1001/jamanetworkopen.2021.0700. JAMA Netw Open. 2021. PMID: 33560421 Free PMC article. No abstract available.
Abstract
Importance: In the pivotal Bevacizumab-Avastin Adjuvant (AVANT) trial, patients with high-risk stage II colon cancer (CC) had 5-year and 10-year overall survival (OS) rates of 88% and 75%, respectively, with adjuvant fluorouracil and oxaliplatin-based chemotherapy; however, the trial did not demonstrate a disease-free survival (DFS) benefit of adding bevacizumab to oxaliplatin-based chemotherapy in stage III CC and suggested a detrimental effect on OS. The Long-term Survival AVANT (S-AVANT) study was designed to collect extended follow-up for patients in the AVANT trial.
Objective: To explore the efficacy of adjuvant bevacizumab combined with oxaliplatin-based chemotherapy in patients with high-risk, stage II CC.
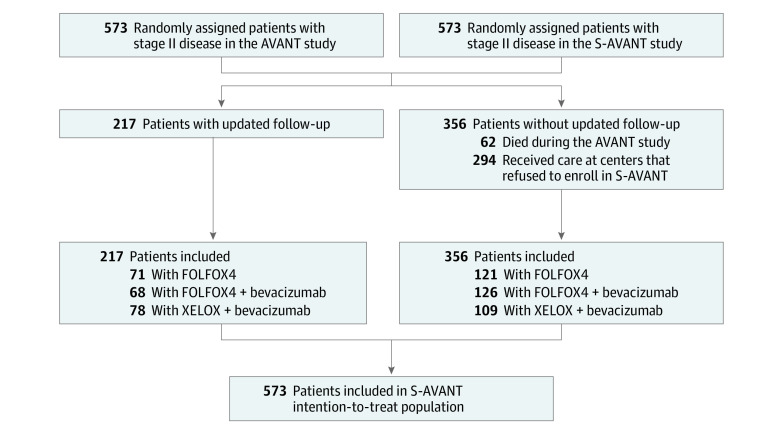
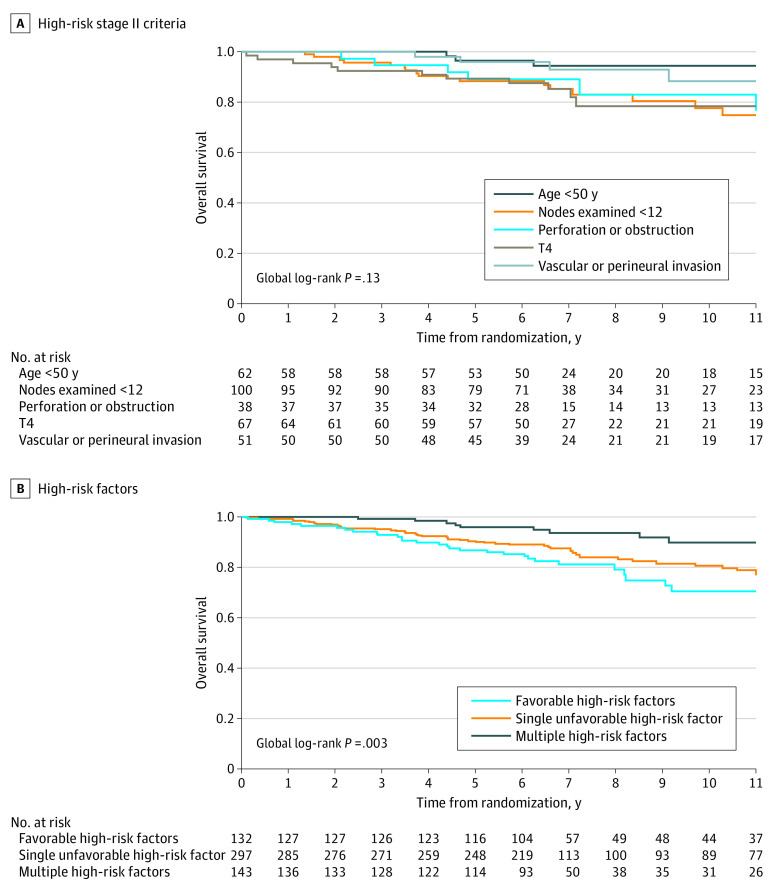
Design, setting, and participants: This prespecified secondary end point analysis of the AVANT and S-AVANT studies included 573 patients with curatively resected high-risk stage II CC and at least 1 of the following criteria: stage T4, bowel obstruction or perforation, blood and/or lymphatic vascular invasion and/or perineural invasion, age younger than 50 years, or fewer than 12 nodes analyzed. The AVANT study was a multicenter randomized stage 3 clinical trial. Data were collected from December 2004 to February 2019, and data for this study were analyzed from March to September 2019.
Intervention: Patients were randomly assigned to receive 5-fluorouracil, leucovorin, and oxaliplatin (FOLFOX4), FOLFOX4 with bevacizumab, or capecitabine and oxaliplatin (XELOX) with bevacizumab.
Main outcomes and measures: The primary end points of this secondary analysis were DFS and OS in patients with high-risk stage II CC.
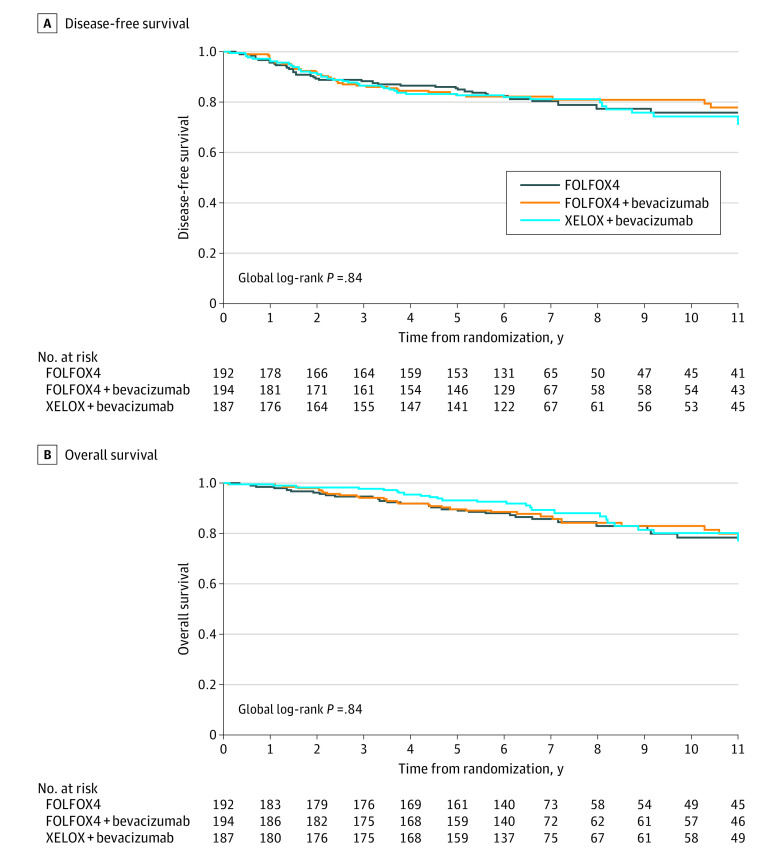
Results: The AVANT study included 3451 patients, of whom 573 (16.6%) had high-risk stage II CC (192 [33.5%] randomized to FOLFOX4 group; 194 [33.9%] randomized to FOLFOX4 with bevacizumab group; 187 [32.6%] randomized to XELOX with bevacizumab group). With a median (interquartile range) age of 57.0 (47.2-65.7) years, the study population comprised 325 men (56.7%) and 248 women (43.3%). After a median (interquartile range) follow-up of 6.9 (6.1-11.3) years, the 3-year DFS and 5-year OS rates were 88.2% (95% CI, 83.7%-93.0%) and 89.7% (95% CI, 85.4%-94.2%) in the FOLFOX4 group, 86.6% (95% CI, 81.8%-91.6%) and 89.7% (95% CI, 85.4%-94.2%) in the FOLFOX4 with bevacizumab group, and 86.7% (95% CI, 81.8%-91.8%) and 93.2% (95% CI, 89.6%-97.0%) in the XELOX with bevacizumab group, respectively. The DFS hazard ratio was 0.94 (95% CI, 0.59-1.48; P = .78) for FOLFOX4 with bevacizumab vs FOLFOX4 and 1.07 (95% CI, 0.69-1.67; P = .76) for XELOX with bevacizumab vs FOLFOX4. The OS hazard ratio was 0.92 (95% CI, 0.55-1.55; P = .76) for FOLFOX4 with bevacizumab vs FOLFOX4 and 0.85 (95% CI, 0.50-1.44; P = .55) for XELOX with bevacizumab vs FOLFOX4.
Conclusions and relevance: In this secondary analysis of data from the AVANT trial, adding bevacizumab to oxaliplatin-based chemotherapy was not associated with longer DFS or OS in patients with high-risk stage II CC. The findings suggest that the definition of high-risk stage II CC needs to be revisited.
Trial registration: ClinicalTrial.gov Identifiers: AVANT (NCT00112918); S-AVANT (NCT02228668).
Conflict of interest statement
Figures
Comment in
-
Antiangiogenesis in Early-Stage Colon Cancer-Microscopically Busted.JAMA Netw Open. 2020 Oct 1;3(10):e2021064. doi: 10.1001/jamanetworkopen.2020.21064. JAMA Netw Open. 2020. PMID: 33074321 No abstract available.
References
-
- André T, Boni C, Mounedji-Boudiaf L, et al. ; Multicenter International Study of Oxaliplatin/5-Fluorouracil/Leucovorin in the Adjuvant Treatment of Colon Cancer (MOSAIC) Investigators . Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350(23):2343-2351. doi: 10.1056/NEJMoa032709 - DOI - PubMed
-
- André T, de Gramont A, Vernerey D, et al. Adjuvant fluorouracil, leucovorin, and oxaliplatin in atage II to III colon cancer: updated 10-year survival and outcomes according to BRAF mutation and mismatch repair status of the MOSAIC Study. J Clin Oncol. 2015;33(35):4176-4187. doi: 10.1200/JCO.2015.63.4238 - DOI - PubMed
