

Gene expression profile predicts response to the combination of tosedostat and low-dose cytarabine in elderly AML
- PMID: 33075137
- PMCID: PMC7594404
- DOI: 10.1182/bloodadvances.2020002305
Gene expression profile predicts response to the combination of tosedostat and low-dose cytarabine in elderly AML
Abstract
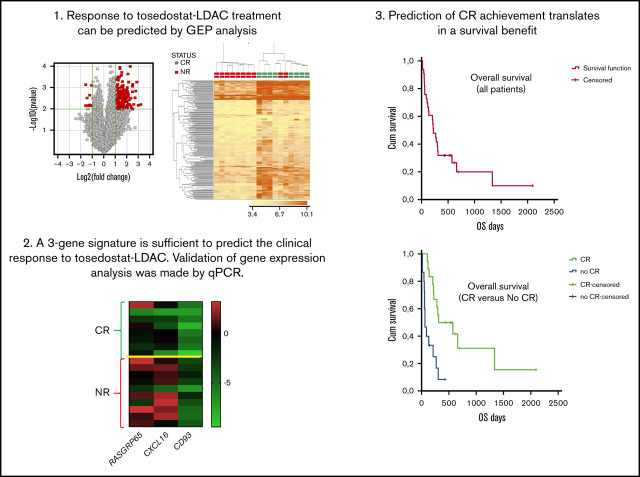
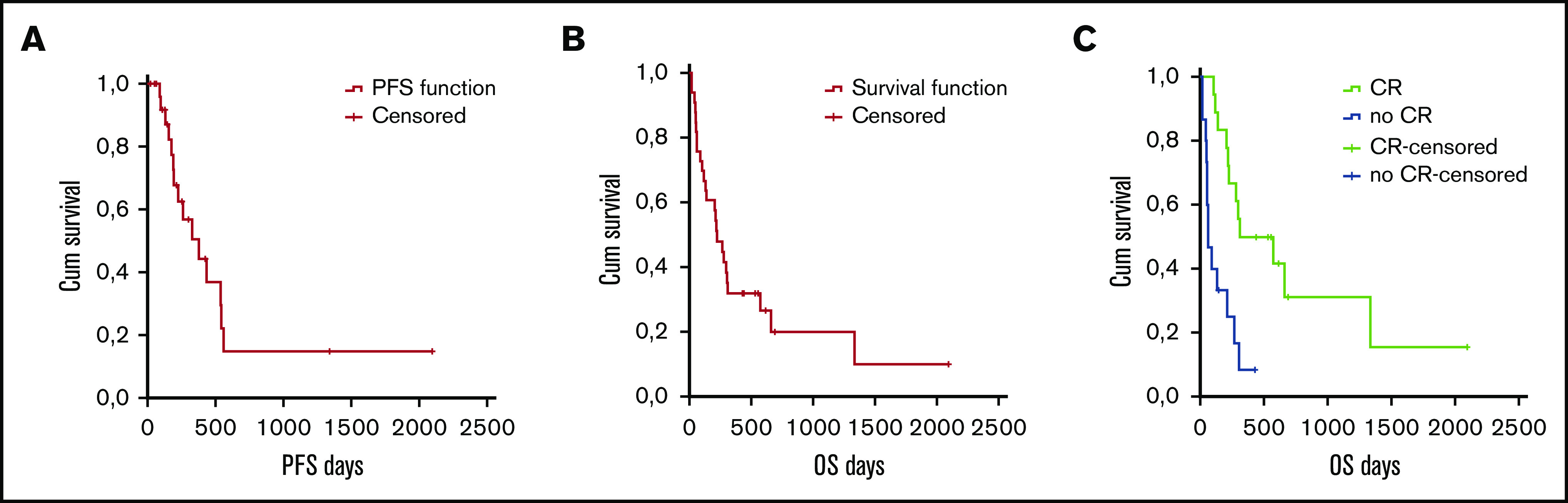
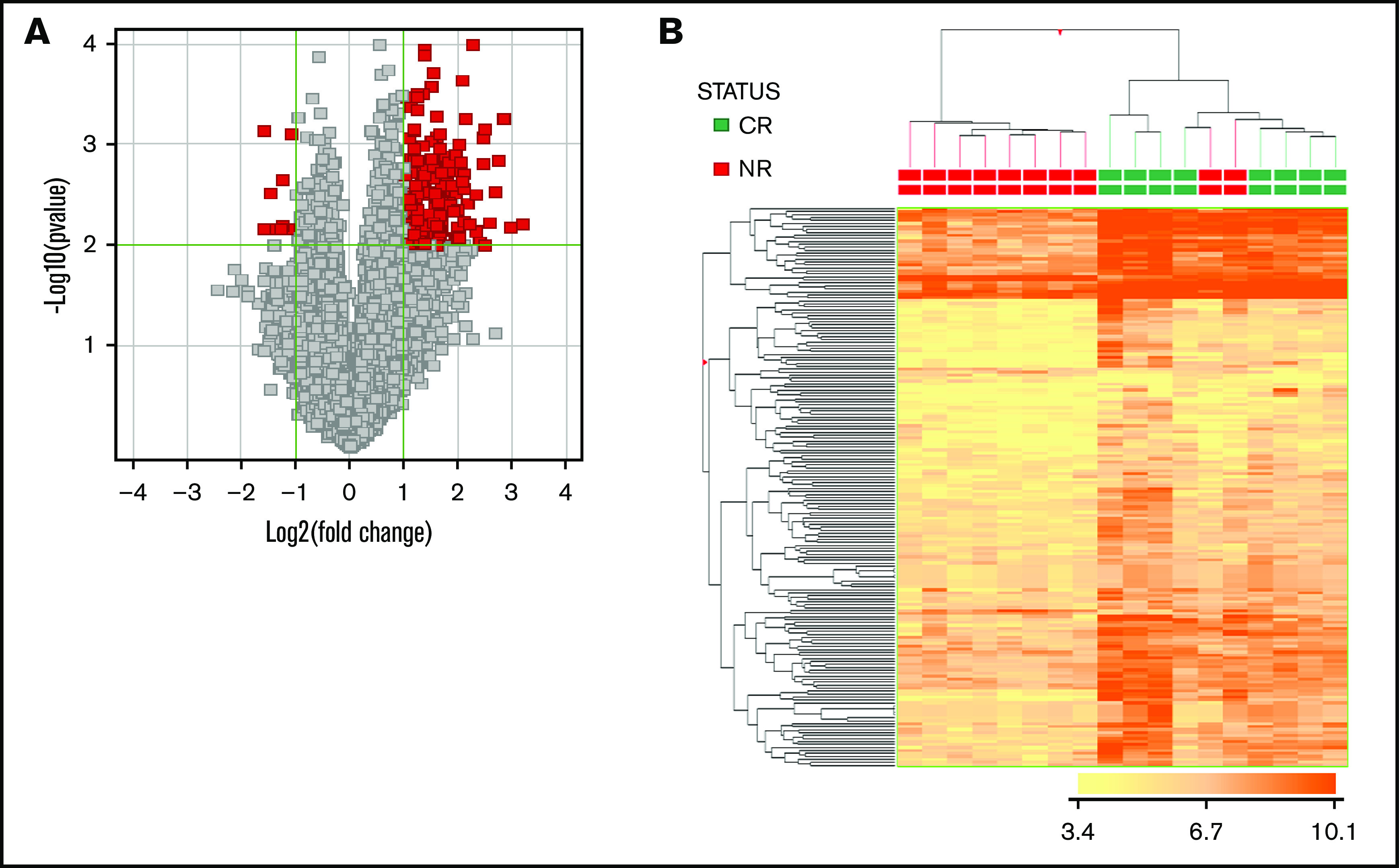
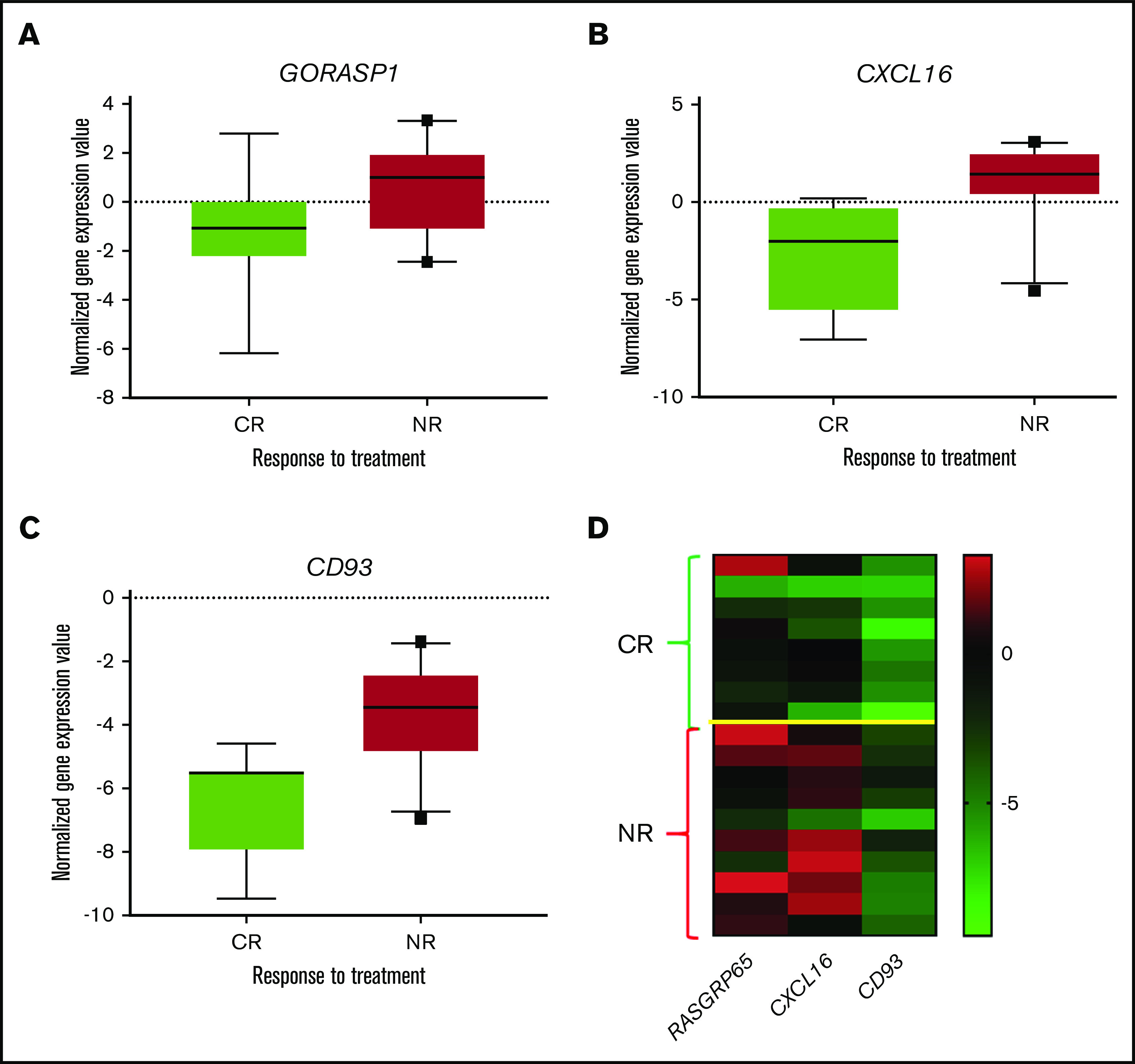
Tosedostat is an orally administered metalloenzyme inhibitor with antiproliferative and antiangiogenic activity against hematological and solid human cancers. Clinical activity has been demonstrated in relapsed acute myeloid leukemia (AML). Thirty-three elderly patients with AML (median age, 75 years) received 120 mg tosedostat orally once daily combined with subcutaneous low-dose cytarabine (20 mg twice per day for 10 days, up to 8 cycles), until disease progression. Induction mortality was 12%. According to an intention-to-treat analysis, the complete remission (CR) rate was 48.5%, and thus the primary end point of the study was reached (expected CR, 25%). The partial remission rate was 6.1%, with an overall response rate of 54.5%. Furthermore, 4 of 33 patients had stable disease (median: 286 days). The median progression-free survival and overall survival (OS) were 203 days and 222 days, respectively. Responding patients had a longer median OS than nonresponding patients (P = .001). A microarray analysis performed in 29 of 33 patients identified 188 genes associated with clinical response (CR vs no CR). Three of them (CD93, GORASP1, CXCL16) were validated by quantitative polymerase chain reaction, which correctly classified 83% of the patients. Specifically, CR achievement was efficiently predicted by the gene expression patterns, with an overall accuracy exceeding 90%. Finally, a negative predictive value of 100% was validated in an independent series, thus representing the first molecular predictor for clinical response to a specific combination drug treatment for AML. This trial has been registered at the European Medicines Agency and on the European Clinical Trials Database (https://www.clinicaltrialsregister.eu) as #2012-000334-19.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures

References
-
- Döhner H, Weisdorf DJ, Bloomfield CD. Acute Myeloid Leukemia. N Engl J Med. 2015;373(12):1136-1152. - PubMed
-
- Leith CP, Kopecky KJ, Godwin J, et al. Acute myeloid leukemia in the elderly: assessment of multidrug resistance (MDR1) and cytogenetics distinguishes biologic subgroups with remarkably distinct responses to standard chemotherapy. A Southwest Oncology Group study. Blood. 1997;89(9):3323-3329. - PubMed
-
- Ossenkoppele G, Löwenberg B. How I treat the older patient with acute myeloid leukemia. Blood. 2015;125(5):767-774. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
