

Comparative Survival Analysis of Immunomodulatory Therapy for Coronavirus Disease 2019 Cytokine Storm
- PMID: 33075378
- PMCID: PMC7567703
- DOI: 10.1016/j.chest.2020.09.275
Comparative Survival Analysis of Immunomodulatory Therapy for Coronavirus Disease 2019 Cytokine Storm
Abstract
Background: Cytokine storm is a marker of coronavirus disease 2019 (COVID-19) illness severity and increased mortality. Immunomodulatory treatments have been repurposed to improve mortality outcomes.
Research question: Do immunomodulatory therapies improve survival in patients with COVID-19 cytokine storm (CCS)?
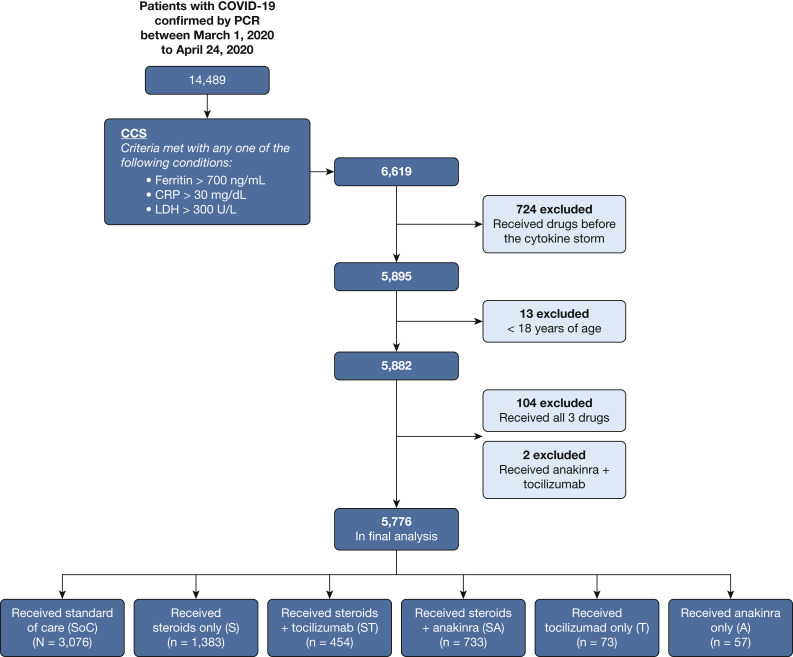
Study design and methods: We conducted a retrospective analysis of electronic health records across the Northwell Health system. COVID-19 patients hospitalized between March 1, 2020, and April 24, 2020, were included. CCS was defined by inflammatory markers: ferritin, > 700 ng/mL; C-reactive protein (CRP), > 30 mg/dL; or lactate dehydrogenase (LDH), > 300 U/L. Patients were subdivided into six groups: no immunomodulatory treatment (standard of care) and five groups that received either corticosteroids, anti-IL-6 antibody (tocilizumab), or anti-IL-1 therapy (anakinra) alone or in combination with corticosteroids. The primary outcome was hospital mortality.
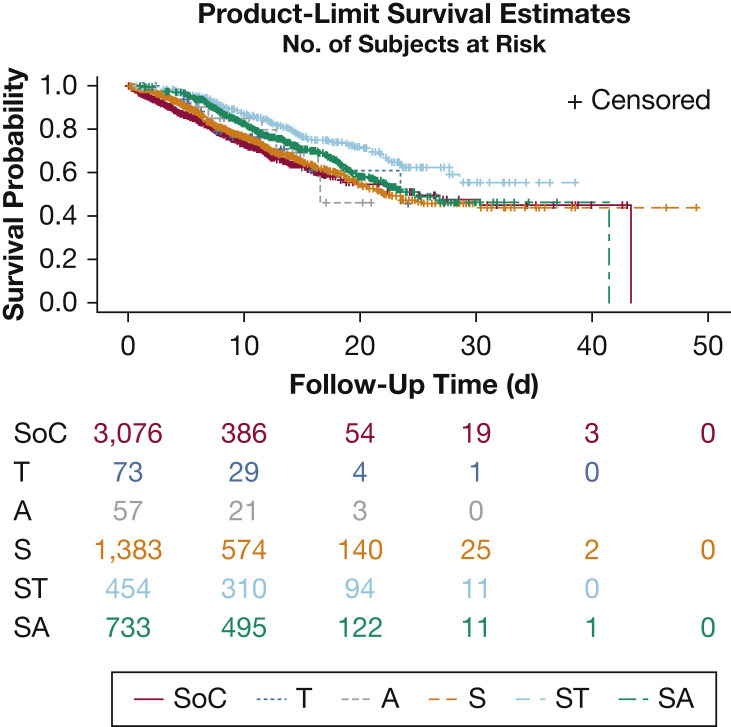
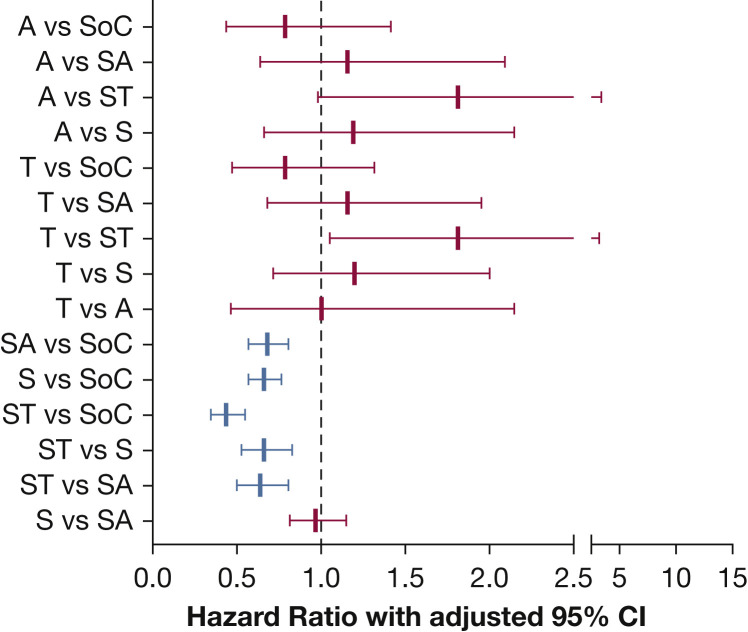
Results: Five thousand seven hundred seventy-six patients met the inclusion criteria. The most common comorbidities were hypertension (44%-59%), diabetes (32%-46%), and cardiovascular disease (5%-14%). Patients most frequently met criteria with high LDH (76.2%) alone or in combination, followed by ferritin (63.2%) and CRP (8.4%). More than 80% of patients showed an elevated D-dimer. Patients treated with corticosteroids and tocilizumab combination showed lower mortality compared with patients receiving standard-of-care (SoC) treatment (hazard ratio [HR], 0.44; 95% CI, 0.35-0.55; P < .0001) and with patients treated with corticosteroids alone (HR, 0.66; 95% CI, 0.53-0.83; P = .004) or in combination with anakinra (HR, 0.64; 95% CI, 0.50-0.81; P = .003). Corticosteroids when administered alone (HR, 0.66; 95% CI, 0.57-0.76; P < .0001) or in combination with tocilizumab (HR, 0.43; 95% CI, 0.35-0.55; P < .0001) or anakinra (HR, 0.68; 95% CI, 0.57-0.81; P < .0001) improved hospital survival compared with SoC treatment.
Interpretation: The combination of corticosteroids with tocilizumab showed superior survival outcome when compared with SoC treatment as well as treatment with corticosteroids alone or in combination with anakinra. Furthermore, corticosteroid use either alone or in combination with tocilizumab or anakinra was associated with reduced hospital mortality for patients with CCS compared with patients receiving SoC treatment.
Keywords: SARS-CoV-2; anakinra; coronavirus; corticosteroids; infection; tocilizumab.
Copyright © 2020 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Corticosteroid Plus Tocilizumab in COVID-19: When Two Is Better Than One.Chest. 2021 May;159(5):2108-2109. doi: 10.1016/j.chest.2020.11.073. Chest. 2021. PMID: 33965134 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
