

Early major recurrence of cerebral aneurysms after satisfactory initial coiling
- PMID: 33076750
- PMCID: PMC8050524
- DOI: 10.1177/1591019920968370
Early major recurrence of cerebral aneurysms after satisfactory initial coiling
Abstract
Background and purpose: Early major recurrence (EMR) of cerebral aneurysms treated by coiling has not been investigated. The purpose of this study is to characterize the frequency and risk factors of this phenomenon.
Materials and methods: A retrospective review was performed of consecutive patients who presented with ruptured and unruptured cerebral aneurysms and underwent coiling from July 2009 to June 2019 at a university hospital. We defined EMR as recurrence of the aneurysm greater than its initial size within the first 6 months of an initial satisfactory coil embolization. Patient demographics, clinical information, aneurysm characteristics, angiographic and technical details were reviewed.
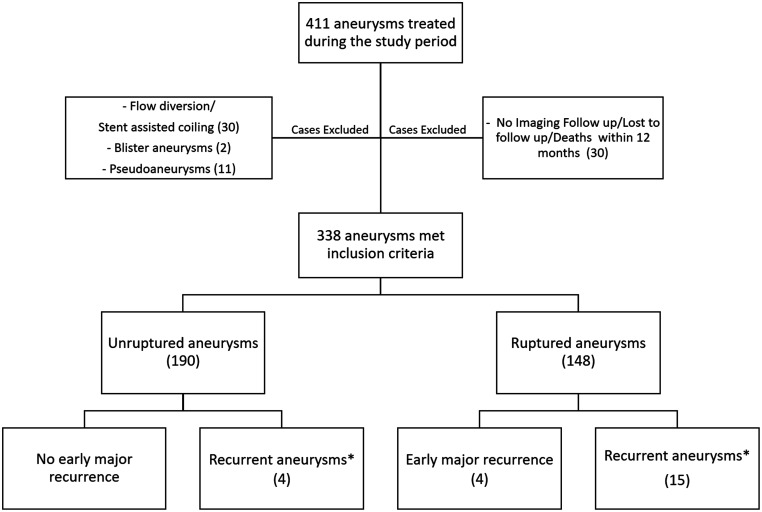
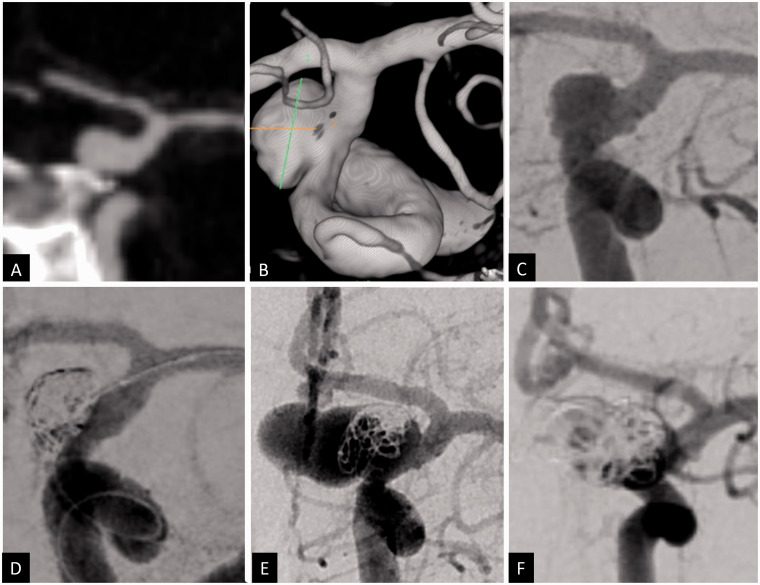
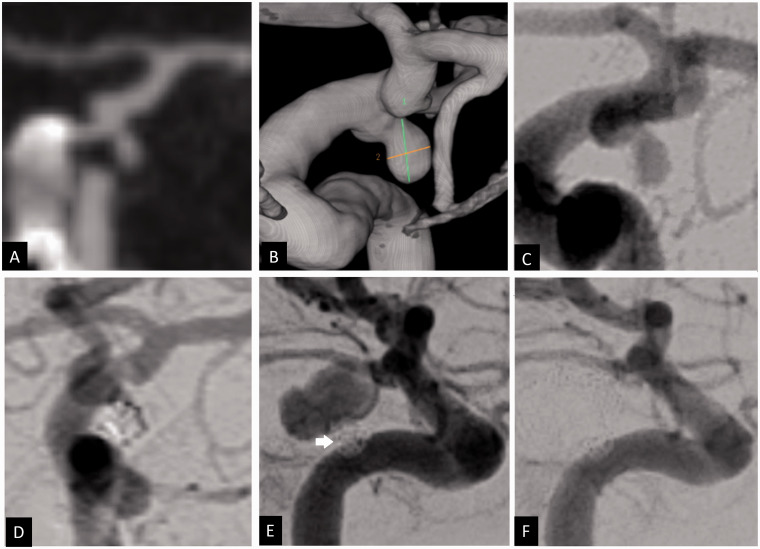
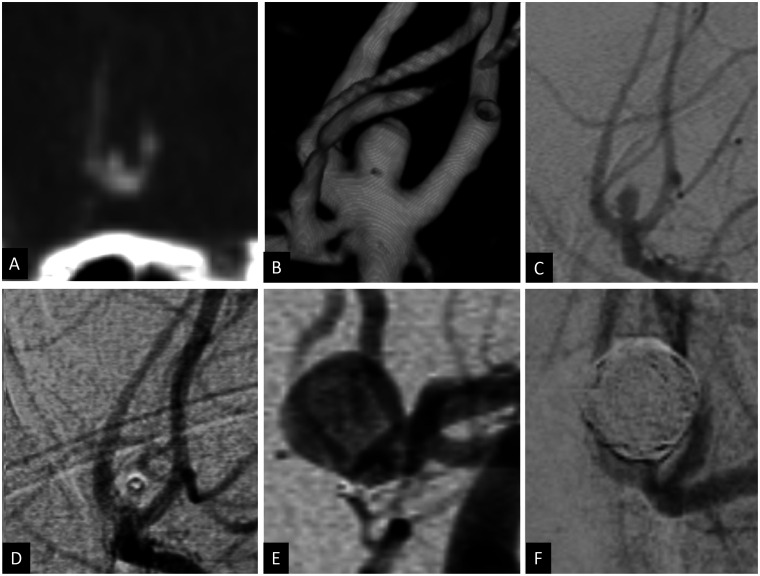
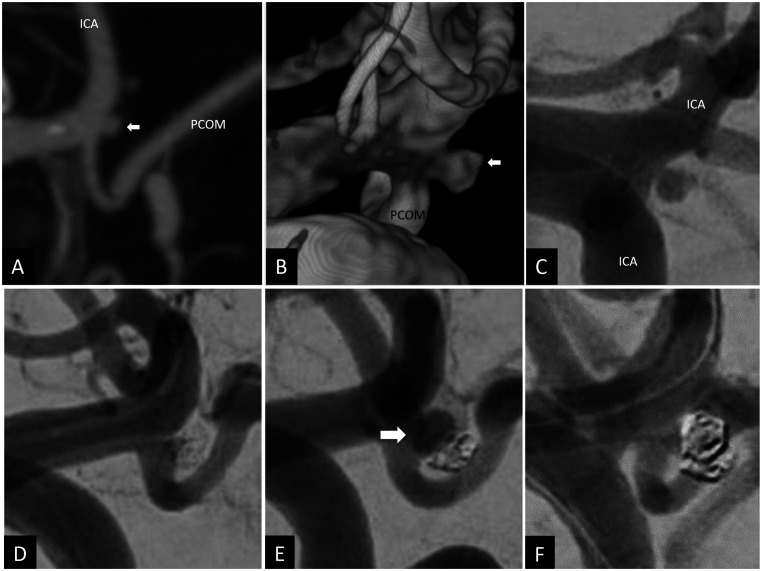
Results: From July 2009 to June 2019, 338 aneurysms (190 unruptured aneurysms and 148 ruptured cerebral aneurysms) underwent coiling and satisfied our study criteria. Among these patients, 23 patients (19 ruptured and 4 unruptured aneurysms) were found to have recurrent aneurysm. Of those, 4 were found to have early major aneurysm regrowth occurring within 6 months after coiling (1.2%). The detection of the EMR was as early as 4 weeks and as late as 20 weeks after the initial coil embolization. The average detection time was 10 ± 7.2 weeks (mean ± SD, range:4-20 weeks). In each case, the recurrent aneurysm cavity was more than twice the initial size of presentation. All aneurysms with major recurrence were ruptured with low aspect ratios (dome height to neck ratio) and involved a communicating segment. All patients underwent successful retreatment of the recurrent aneurysm with good outcome.
Conclusions: Early major recurrence of treated aneurysms is a rare but important complication that harbors an impending risk of re-rupture. Early control angiography after endovascular coiling may be warranted for small ruptured aneurysms, even in cases in which the initial result seems technically satisfactory.
Keywords: Recurrence; endovascular coiling; ruptured aneurysm; subarachnoid hemorrhage.
Conflict of interest statement
Figures
References
-
- Lecler A, Raymond J, Rodriguez-Régent C, et al. Intracranial aneurysms: recurrences more than 10 years after endovascular treatment – a prospective cohort study, systematic review, and meta-analysis. Radiology 2015; 277: 173–180. - PubMed
-
- Raymond J, Guilbert Fois, Weill Alain, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke 2003; 34: 1398–1403. - PubMed
-
- The CARAT Investigators. Rates of delayed rebleeding from intracranial aneurysms are low after surgical and endovascular treatment. Stroke 2006; 37: 1437–1442. - PubMed
-
- Campi A, Ramzi N, Molyneux AJ, et al. Retreatment of ruptured cerebral aneurysms in patients randomized by coiling or clipping in the international subarachnoid aneurysm trial (ISAT). Stroke 2007; 38: 1538–1544. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
