

Examining the pace of change in contraceptive practices in abortion services - a follow-up case study of a quality improvement collaborative
- PMID: 33076890
- PMCID: PMC7574423
- DOI: 10.1186/s12913-020-05799-x
Examining the pace of change in contraceptive practices in abortion services - a follow-up case study of a quality improvement collaborative
Abstract
Background: Among all women who experienced an abortion in Sweden 2017, 45% had previously underwent at least one abortion. This phenomenon of increasing rates of repeat abortions stimulated efforts to improve contraceptive services through a Quality Improvement Collaborative (QIC) with user involvement. The participating teams had difficulty in coordinating access post-abortion to the most effective contraception, Long-acting reversible contraception (LARC), during the eight-month QIC. This prompted questions about the pace of change in contraceptive services post-abortion. The aim of the study is to evaluate the evolution and impact of QIC changes regarding patient outcomes, system performance and professional development over 12 months after a QIC designed to enhance contraceptive services in the context of abortion.
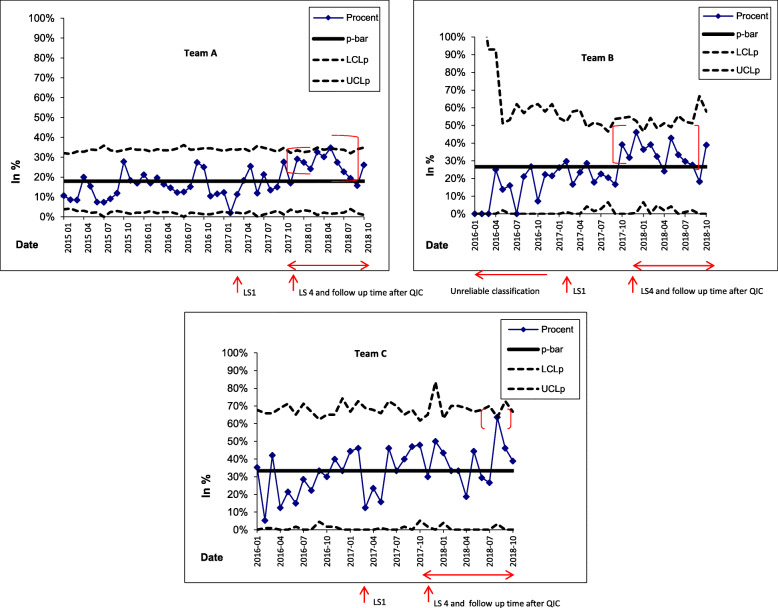
Methods: This follow-up case study involves three multi-professional teams from abortion services at three hospitals in Sweden, which participated in a QIC during 2017. We integrated qualitative data on the evolution of changes and quantitative data regarding the monthly proportion of women initiating LARC, analysed in statistical control charts from before the QIC up until 12 months after its conclusion.
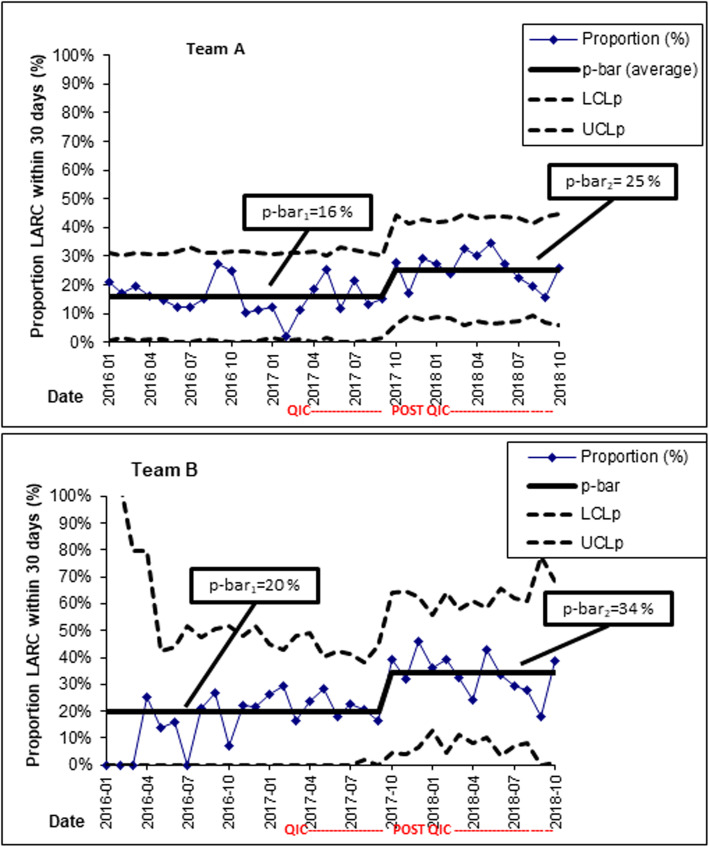
Results: Teams A and B increased the average proportion of women who initiated LARC within 30 days post abortion in the 12 months after the QIC; Team A 16-25%; Team B 20-34%. Team C achieved more than 50% in individual months but not consistently in the Post-QIC period. Elusive during the QIC, they now could offer timely appointments for women to initiate LARC more frequently. Team members reported continued focus on how to create trustful relationships when counseling women. They described improved teamwork, leadership support and impact on organizing appointments for initiating LARC following the QIC.
Conclusions: QIC teams further improved women's timely access to LARC post abortion through continued changes in services 12 months after the QIC, demonstrating that the 8-month QIC was too short for all changes to materialize. Teams simultaneously improved women's reproductive health, health services, and professional development.
Keywords: Contraceptive counselling; Health services accessibility; Long- acting reversible contraception; Professional development and pregnancy termination; Quality improvement; System performance.
Conflict of interest statement
Two of the co-authors have been reimbursed by Merck Sharpe & Dohme Bayer AB Sweden (JB, HK) and Actavis (JB) for running educational programmes and giving lectures. The other co-authors have stated that they have no conflicts of interest in connection with this manuscript.
Figures
Similar articles
-
Developing contraceptive services for immigrant women postpartum - a case study of a quality improvement collaborative in Sweden.BMC Health Serv Res. 2022 Apr 26;22(1):556. doi: 10.1186/s12913-022-07965-9. BMC Health Serv Res. 2022. PMID: 35473622 Free PMC article.
-
Collaboratively seeking to improve contraceptive counselling at the time of an abortion: a case study of quality improvement efforts in Sweden.BMJ Sex Reprod Health. 2019 Jul;45(3):190-199. doi: 10.1136/bmjsrh-2018-200299. BMJ Sex Reprod Health. 2019. PMID: 31289100
-
Risk factors and the choice of long-acting reversible contraception following medical abortion: effect on subsequent induced abortion and unwanted pregnancy.Eur J Contracept Reprod Health Care. 2018 Apr;23(2):89-96. doi: 10.1080/13625187.2018.1440385. Epub 2018 Mar 14. Eur J Contracept Reprod Health Care. 2018. PMID: 29537321
-
Canadian Contraception Consensus (Part 1 of 4).J Obstet Gynaecol Can. 2015 Oct;37(10):936-42. doi: 10.1016/s1701-2163(16)30033-0. J Obstet Gynaecol Can. 2015. PMID: 26606712 English, French.
-
Uptake of long-acting reversible contraception after telemedicine delivered abortion during Covid-19.Eur J Contracept Reprod Health Care. 2022 Aug;27(4):284-288. doi: 10.1080/13625187.2022.2085680. Epub 2022 Jun 17. Eur J Contracept Reprod Health Care. 2022. PMID: 35713651 Review.
Cited by
-
What factors influence a Quality Improvement Collaborative in improving contraceptive services for foreign-born women? A qualitative study in Sweden.BMC Health Serv Res. 2023 Oct 11;23(1):1089. doi: 10.1186/s12913-023-10060-2. BMC Health Serv Res. 2023. PMID: 37821891 Free PMC article.
-
Developing contraceptive services for immigrant women postpartum - a case study of a quality improvement collaborative in Sweden.BMC Health Serv Res. 2022 Apr 26;22(1):556. doi: 10.1186/s12913-022-07965-9. BMC Health Serv Res. 2022. PMID: 35473622 Free PMC article.
-
IMplementing best practice post-partum contraceptive services through a quality imPROVEment initiative for and with immigrant women in Sweden (IMPROVE it): a protocol for a cluster randomised control trial with a process evaluation.BMC Public Health. 2023 May 3;23(1):806. doi: 10.1186/s12889-023-15776-8. BMC Public Health. 2023. PMID: 37138268 Free PMC article.
References
-
- Benson J, Andersen K, Brahmi D, Healy J, Mark A, Ajode A, et al. What contraception do women use after abortion? An analysis of 319,385 cases from eight countries. Glob Public Health. 2016;18:1–16. - PubMed
-
- World Health Organization . Sexual health and its linkages to reproductive health: an operational approach. 2017.
-
- Socialstyrelsen . Abortstatistik. 2018.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
