

Multiple myeloma and SARS-CoV-2 infection: clinical characteristics and prognostic factors of inpatient mortality
- PMID: 33077708
- PMCID: PMC7570395
- DOI: 10.1038/s41408-020-00372-5
Multiple myeloma and SARS-CoV-2 infection: clinical characteristics and prognostic factors of inpatient mortality
Abstract
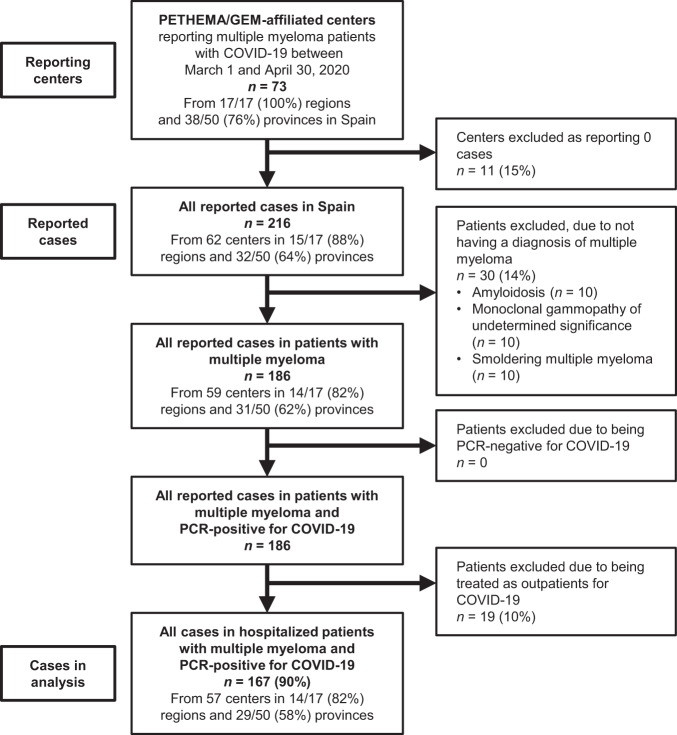
There is limited information on the characteristics, prognostic factors, and outcomes of patients with multiple myeloma (MM) hospitalized with COVID-19. This retrospective case series investigated 167 patients reported from 73 hospitals within the Spanish Myeloma Collaborative Group network in March and April, 2020. Outcomes were compared with 167 randomly selected, contemporary, age-/sex-matched noncancer patients with COVID-19 admitted at six participating hospitals. Among MM and noncancer patients, median age was 71 years, and 57% of patients were male; 75 and 77% of patients, respectively, had at least one comorbidity. COVID-19 clinical severity was moderate-severe in 77 and 89% of patients and critical in 8 and 4%, respectively. Supplemental oxygen was required by 47 and 55% of MM and noncancer patients, respectively, and 21%/9% vs 8%/6% required noninvasive/invasive ventilation. Inpatient mortality was 34 and 23% in MM and noncancer patients, respectively. Among MM patients, inpatient mortality was 41% in males, 42% in patients aged >65 years, 49% in patients with active/progressive MM at hospitalization, and 59% in patients with comorbid renal disease at hospitalization, which were independent prognostic factors on adjusted multivariate analysis. This case series demonstrates the increased risk and identifies predictors of inpatient mortality among MM patients hospitalized with COVID-19.
Conflict of interest statement
M.-V.M. has received honoraria for lectures and participation in advisory boards from Janssen, Celgene-BMS, Amgen, Takeda, Abbvie, GSK, Adaptive, Roche, Seatle Genetics, Pfizer, and Regeneron. J.M.-L. has received honoraria for participation in advisory boards from Novartis, Roche, BMS, Adaptive, Incyte, Amgen, and Janssen-Cilag. J.S.-M. has received honoraria for lectures and advisory boards from Amgen, Bristol–Myers Squibb, Celgene, Janssen, Merck, Novartis, Takeda, Sanofi, and Roche. J.B. has received honoraria for lectures and advisory boards from Janssen, Celgene, Amgen, Takeda, and Oncopeptides. J.J.L. has received honoraria for lectures and advisory boards from Janssen, Celgene, Amgen, and Takeda. A.L. has received honoraria for advisory boards from Celgene, Amgen, and Janssen. P.M.-B. has received honoraria for advisory boards from Amgen. A.S. has received honoraria for advisory boards from Takeda, BMS, MSD, Sanofi, Roche, Novartis, Janssen, and Sandoz, and for a consultancy from Takeda, BMS, Novartis, Celgene, Janssen, Gilead, and Sanofi, and has received honoraria as a member of a Speakers Bureau for Takeda. F.E. has received honoraria for advisory boards from Celgene and Amgen. E.P.P. has received honoraria for advisory boards from Amgen and for lectures from BMS/Celgene and Janssen. C.F.d.L. has received honoraria for advisory boards from BMS/Celgene, Amgen, Takeda, and Janssen. L.F.C. reports honoraria for lectures from and membership on advisory boards with Celgene, Janssen, Roche, Novartis, Bristol–Myers Squibb, Amgen, Takeda, Pfizer, Incyte, and AbbVie. The remaining authors declare that they have no conflict of interest.
Figures
References
-
- World Health Organization. Novel Coronavirus–China. World Health Organization.https://www.who.int/china/news/detail/09-01-2020-who-statement-regarding... (WHO, 2020).
