

Immunity, endothelial injury and complement-induced coagulopathy in COVID-19
- PMID: 33077917
- PMCID: PMC7570423
- DOI: 10.1038/s41581-020-00357-4
Immunity, endothelial injury and complement-induced coagulopathy in COVID-19
Abstract
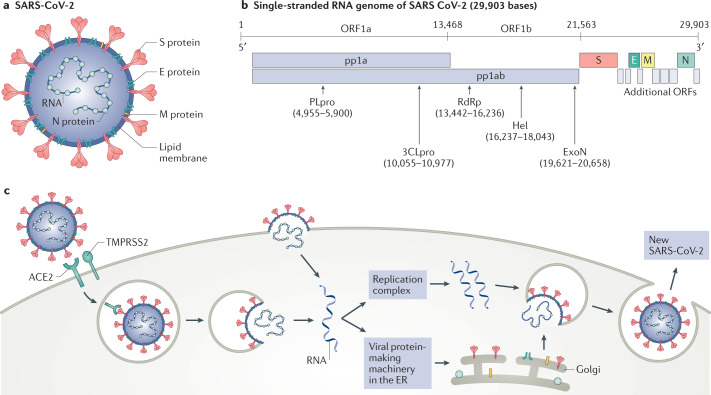
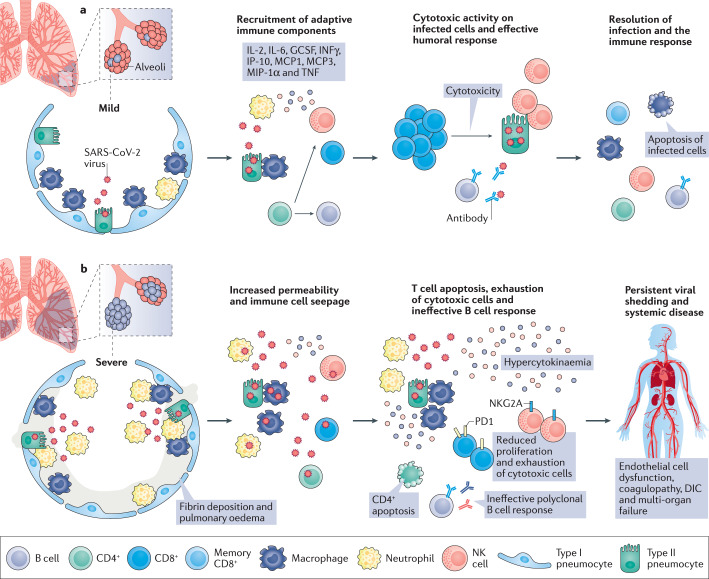
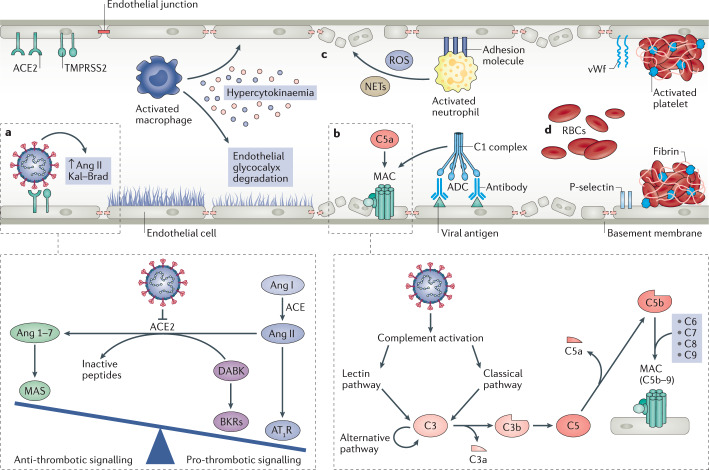
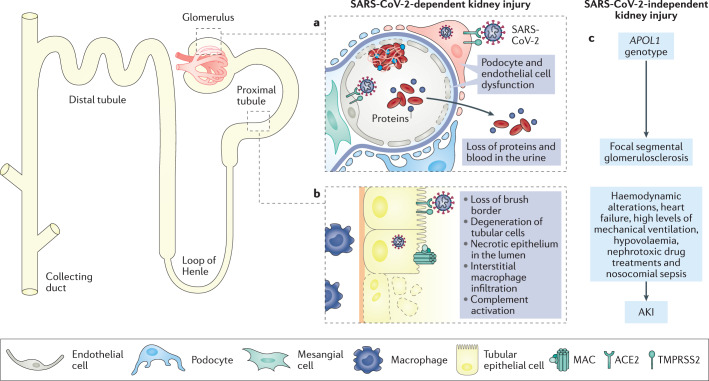
In December 2019, a novel coronavirus was isolated from the respiratory epithelium of patients with unexplained pneumonia in Wuhan, China. This pathogen, named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), causes a pathogenic condition that has been termed coronavirus disease 2019 (COVID-19) and has reached pandemic proportions. As of 17 September 2020, more than 30 million confirmed SARS-CoV-2 infections have been reported in 204 different countries, claiming more than 1 million lives worldwide. Accumulating evidence suggests that SARS-CoV-2 infection can lead to a variety of clinical conditions, ranging from asymptomatic to life-threatening cases. In the early stages of the disease, most patients experience mild clinical symptoms, including a high fever and dry cough. However, 20% of patients rapidly progress to severe illness characterized by atypical interstitial bilateral pneumonia, acute respiratory distress syndrome and multiorgan dysfunction. Almost 10% of these critically ill patients subsequently die. Insights into the pathogenic mechanisms underlying SARS-CoV-2 infection and COVID-19 progression are emerging and highlight the critical role of the immunological hyper-response - characterized by widespread endothelial damage, complement-induced blood clotting and systemic microangiopathy - in disease exacerbation. These insights may aid the identification of new or existing therapeutic interventions to limit the progression of early disease and treat severe cases.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
