

Neuroinflammation after surgery: from mechanisms to therapeutic targets
- PMID: 33077953
- PMCID: PMC7704062
- DOI: 10.1038/s41590-020-00812-1
Neuroinflammation after surgery: from mechanisms to therapeutic targets
Abstract
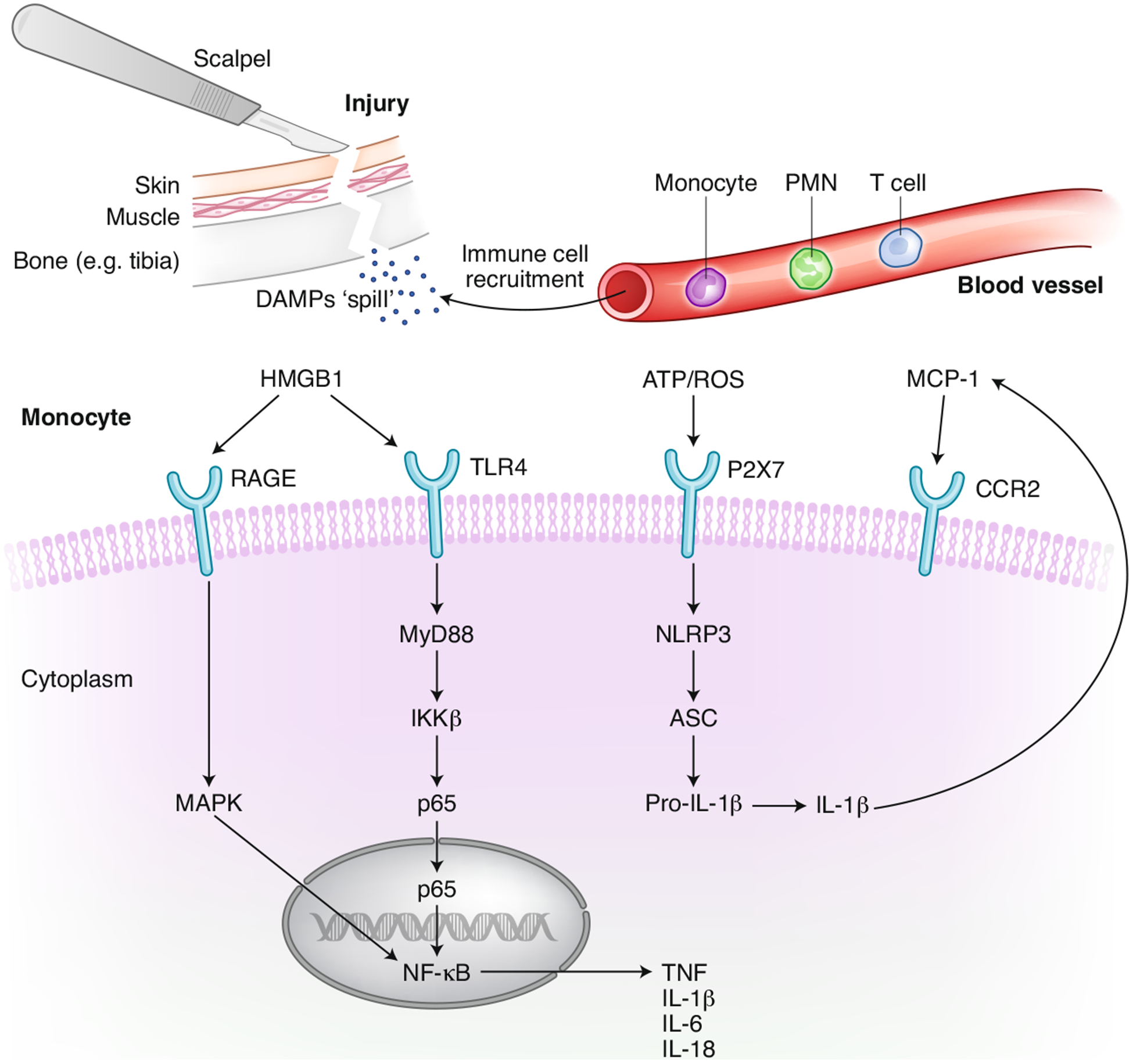
Injury is a key driver of inflammation, a critical yet necessary response involving several mediators that is aimed at restoring tissue homeostasis. Inflammation in the central nervous system can be triggered by a variety of stimuli, some intrinsic to the brain and others arising from peripheral signals. Fine-tuned regulation of this response is crucial in a system that is vulnerable due to, for example, aging and ongoing neurodegeneration. In this context, seemingly harmless interventions like a common surgery to repair a broken limb can overwhelm the immune system and become the driver of further complications such as delirium and other perioperative neurocognitive disorders. Here, we discuss potential mechanisms by which the immune system affects the central nervous system after surgical trauma. Together, these neuroimmune interactions are becoming hallmarks of and potential therapeutic targets for multiple neurologic conditions, including those affecting the perioperative space.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures

References
-
- Pluvinage JV & Wyss-Coray T Systemic factors as mediators of brain homeostasis, ageing and neurodegeneration. Nat. Rev. Neurosci 21, 93–102 (2020). - PubMed
-
- Gelderblom M et al. Temporal and spatial dynamics of cerebral immune cell accumulation in stroke. Stroke 40, 1849–1857 (2009). - PubMed
-
- Evered L & Eckenhoff RG & International Perioperative Cognition Nomenclature Working Group. Perioperative cognitive disorders. Response to: postoperative delirium portends descent to dementia. Br. J. Anaesth 119, 1241 (2017). - PubMed
-
- Evered LA & Silbert BS Postoperative cognitive dysfunction and noncardiac surgery. Anesth. Analg 127, 496–505 (2018). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
