

Breath-, air- and surface-borne SARS-CoV-2 in hospitals
- PMID: 33078030
- PMCID: PMC7557302
- DOI: 10.1016/j.jaerosci.2020.105693
Breath-, air- and surface-borne SARS-CoV-2 in hospitals
Abstract
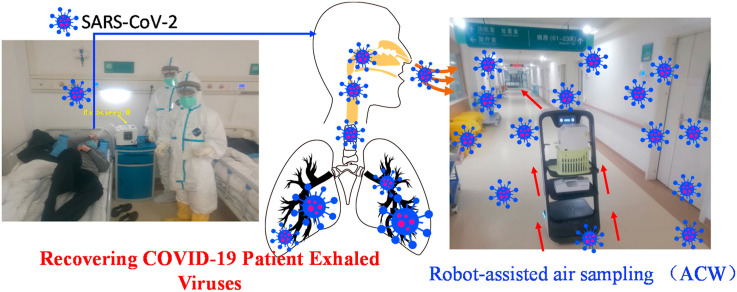
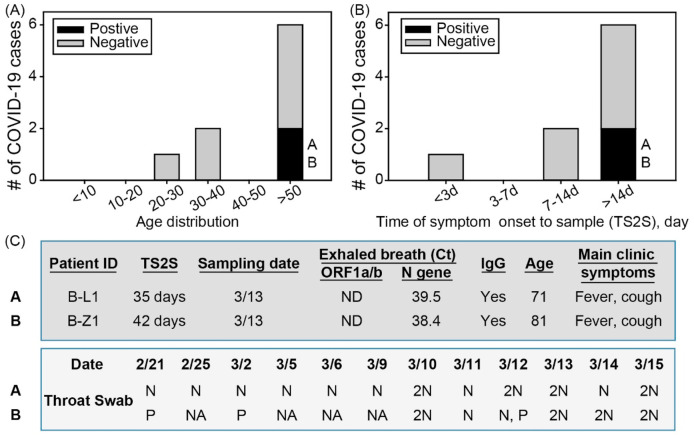
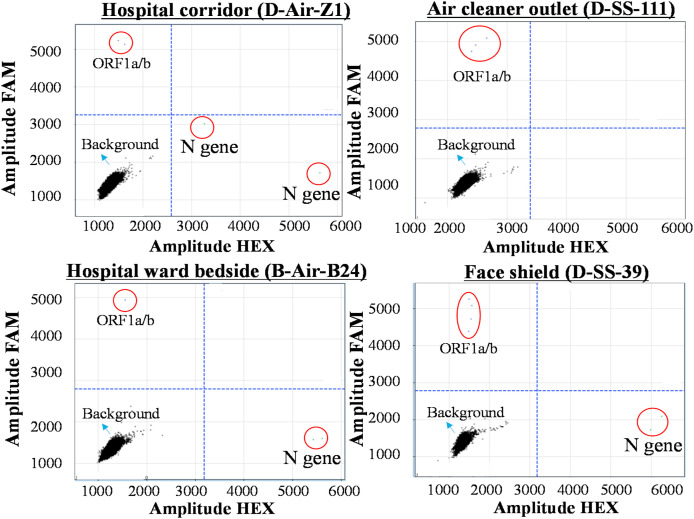
The COVID-19 pandemic has brought an unprecedented crisis to the global health sector. When discharging COVID-19 patients in accordance with throat or nasal swab protocols using RT-PCR, the potential risk of reintroducing the infection source to humans and the environment must be resolved. Here, 14 patients including 10 COVID-19 subjects were recruited; exhaled breath condensate (EBC), air samples and surface swabs were collected and analyzed for SARS-CoV-2 using reverse transcription-polymerase chain reaction (RT-PCR) in four hospitals with applied natural ventilation and disinfection practices in Wuhan. Here we discovered that 22.2% of COVID-19 patients (n = 9), who were ready for hospital discharge based on current guidelines, had SARS-CoV-2 in their exhaled breath (~105 RNA copies/m3). Although fewer surface swabs (3.1%, n = 318) tested positive, medical equipment such as face shield frequently contacted/used by healthcare workers and the work shift floor were contaminated by SARS-CoV-2 (3-8 viruses/cm2). Three of the air samples (n = 44) including those collected using a robot-assisted sampler were detected positive by a digital PCR with a concentration level of 9-219 viruses/m3. RT-PCR diagnosis using throat swab specimens had a failure rate of more than 22% in safely discharging COVID-19 patients who were otherwise still exhaling the SARS-CoV-2 by a rate of estimated ~1400 RNA copies per minute into the air. Direct surface contact might not represent a major transmission route, and lower positive rate of air sample (6.8%) was likely due to natural ventilation (1.6-3.3 m/s) and regular disinfection practices. While there is a critical need for strengthening hospital discharge standards in preventing re-emergence of COVID-19 spread, use of breath sample as a supplement specimen could further guard the hospital discharge to ensure the safety of the public and minimize the pandemic re-emergence risk.
Keywords: Airborne transmission; COVID-19; Exhaled breath; SARS-CoV-2; Surface-borne.
© 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- van Doremalen N., Bushmaker T., Morris D.H., Holbrook M.G., Gamble A., Williamson B.N., Tamin A., Harcourt J.L., Thornburg N.J., Gerber S.I., Lloyd-Smith J.O., de Wit E., Munster V.J. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. New England Journal of Medicine. 2020;382:1564–1567. - PMC - PubMed
-
- Epidemiology Working Group for NCIP Epidemic Response, Chinese Center for Disease Prevention and Control (CCDC) The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China, 2020. Chinese Journal of Epidemiology. 2020;41:145–151.
-
- Guo Z.D., Wang Z.Y., Zhang S.F., Li X., Li L., Li C., Cui Y., Fu R., Dong Y., Chi X., Zhang M., Liu K., Cao C., Liu B., Zhang K., Gao Y., Lu B., Chen W. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerging Infectious Diseases. 2020;26(7):1583–1591. - PMC - PubMed
-
- Lednicky J.A., Lauzardo M., Fan Z.H., Jutla A., Tilly T.B., Gangwar M., Usmani M., Shankar S.N., Mohamed K., Eiguren-Fernandez A., Stephenson C.J., Alam M.M., Elbadry M.A., Loeb J.C., Subramaniam K., Waltzek T.B., Cherabuddi K., Morris G.J., Wu C.Y. Viable SARS-CoV-2 in the air of a hospital room with COVID-19 patients. International Journal of Infectious Diseases. 2020 doi: 10.1016/j.ijid.2020.09.025. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous