

Machine Learning to Develop and Internally Validate a Predictive Model for Post-operative Delirium in a Prospective, Observational Clinical Cohort Study of Older Surgical Patients
- PMID: 33078300
- PMCID: PMC7878663
- DOI: 10.1007/s11606-020-06238-7
Machine Learning to Develop and Internally Validate a Predictive Model for Post-operative Delirium in a Prospective, Observational Clinical Cohort Study of Older Surgical Patients
Abstract
Background: Our objective was to assess the performance of machine learning methods to predict post-operative delirium using a prospective clinical cohort.
Methods: We analyzed data from an observational cohort study of 560 older adults (≥ 70 years) without dementia undergoing major elective non-cardiac surgery. Post-operative delirium was determined by the Confusion Assessment Method supplemented by a medical chart review (N = 134, 24%). Five machine learning algorithms and a standard stepwise logistic regression model were developed in a training sample (80% of participants) and evaluated in the remaining hold-out testing sample. We evaluated three overlapping feature sets, restricted to variables that are readily available or minimally burdensome to collect in clinical settings, including interview and medical record data. A large feature set included 71 potential predictors. A smaller set of 18 features was selected by an expert panel using a consensus process, and this smaller feature set was considered with and without a measure of pre-operative mental status.
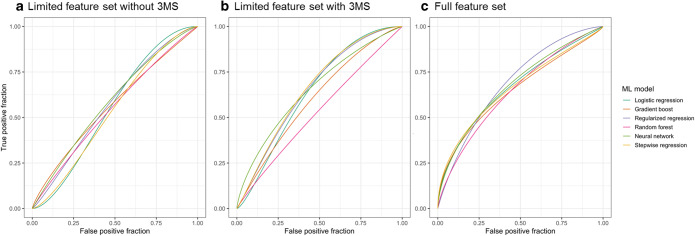
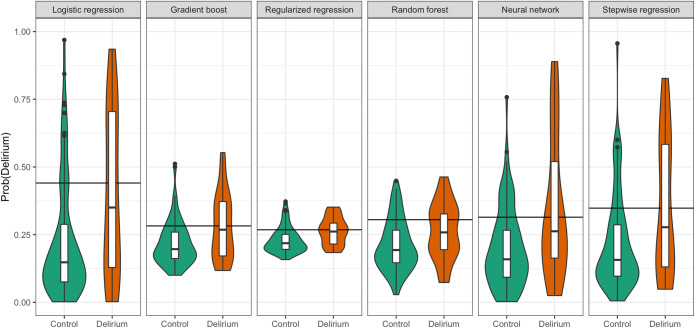
Results: The area under the receiver operating characteristic curve (AUC) was higher in the large feature set conditions (range of AUC, 0.62-0.71 across algorithms) versus the selected feature set conditions (AUC range, 0.53-0.57). The restricted feature set with mental status had intermediate AUC values (range, 0.53-0.68). In the full feature set condition, algorithms such as gradient boosting, cross-validated logistic regression, and neural network (AUC = 0.71, 95% CI 0.58-0.83) were comparable with a model developed using traditional stepwise logistic regression (AUC = 0.69, 95% CI 0.57-0.82). Calibration for all models and feature sets was poor.
Conclusions: We developed machine learning prediction models for post-operative delirium that performed better than chance and are comparable with traditional stepwise logistic regression. Delirium proved to be a phenotype that was difficult to predict with appreciable accuracy.
Keywords: delirium; machine learning; model prediction; post-operative; statistical learning.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
- R03AG061582/AG/NIA NIH HHS/United States
- T32AG023480/AG/NIA NIH HHS/United States
- R03 AG061582/AG/NIA NIH HHS/United States
- K24 AG035075/AG/NIA NIH HHS/United States
- K07 AG041835/AG/NIA NIH HHS/United States
- AARF-18-560786/ALZ/Alzheimer's Association/United States
- R24 AG054259/AG/NIA NIH HHS/United States
- K24AG035075/AG/NIA NIH HHS/United States
- T32 AG023480/AG/NIA NIH HHS/United States
- R01 AG044518/AG/NIA NIH HHS/United States
- R01AG03061/AG/NIA NIH HHS/United States
- K01AG057836/AG/NIA NIH HHS/United States
- R24AG054259/AG/NIA NIH HHS/United States
- K07AG041835/AG/NIA NIH HHS/United States
- K01 AG057836/AG/NIA NIH HHS/United States
- P01AG031720/AG/NIA NIH HHS/United States
- P01 AG031720/AG/NIA NIH HHS/United States
- R01AG04451/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
